ECG Acquisition, Transmission & Interpretation
ECG Acquisition, Transmission & Interpretation
(3 Leads ECG)
EMTs can apply 3 lead ECG to patient direct on-scene where there no Paramedic available. Strongly encouraged to develop the capability to transmit ECGs to receiving hospitals.
STANDING ORDERS:-
Obtain 3-lead ECG with baseline vitals within 10 minutes for potential ACS if available and practical and transmit per local guidelines.
INDICATIONS:-
- Dysrhythmias, palpitations.
- Suspected Acute Coronary Syndrome (chest, jaw, arm, or epigastric discomfort, diaphoresis, weakness).
- Syncope.
- Shortness of breath.
- Congestive Heart Failure/Pulmonary Edema.
PROCEDURE:-
- Prepare ECG Monitor and connect cable with electrodes.
- Properly position the patient (supine or semi-reclined).
- Enter patient information (e.g. age, gender) into monitor.
- Prep chest as necessary, (e.g. hair removal, skin prep pads).
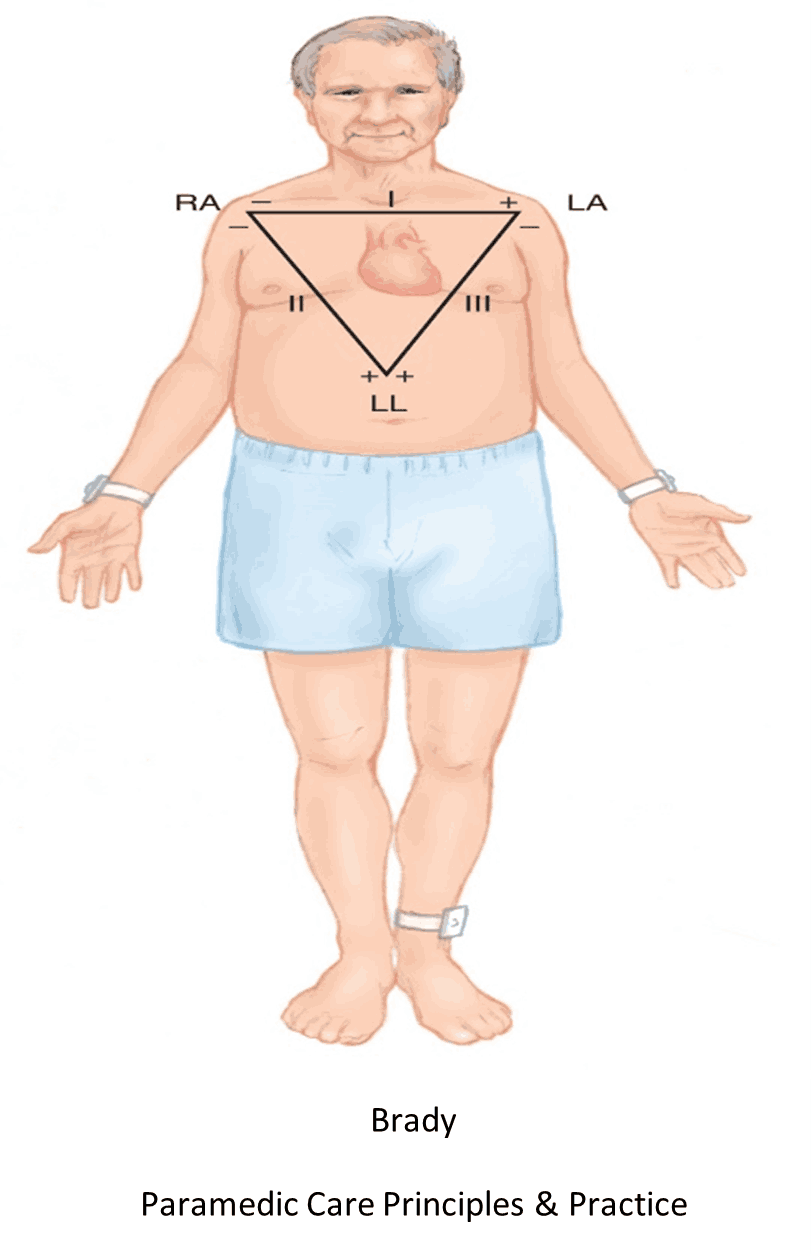
- Apply chest and extremity leads using recommended landmarks:
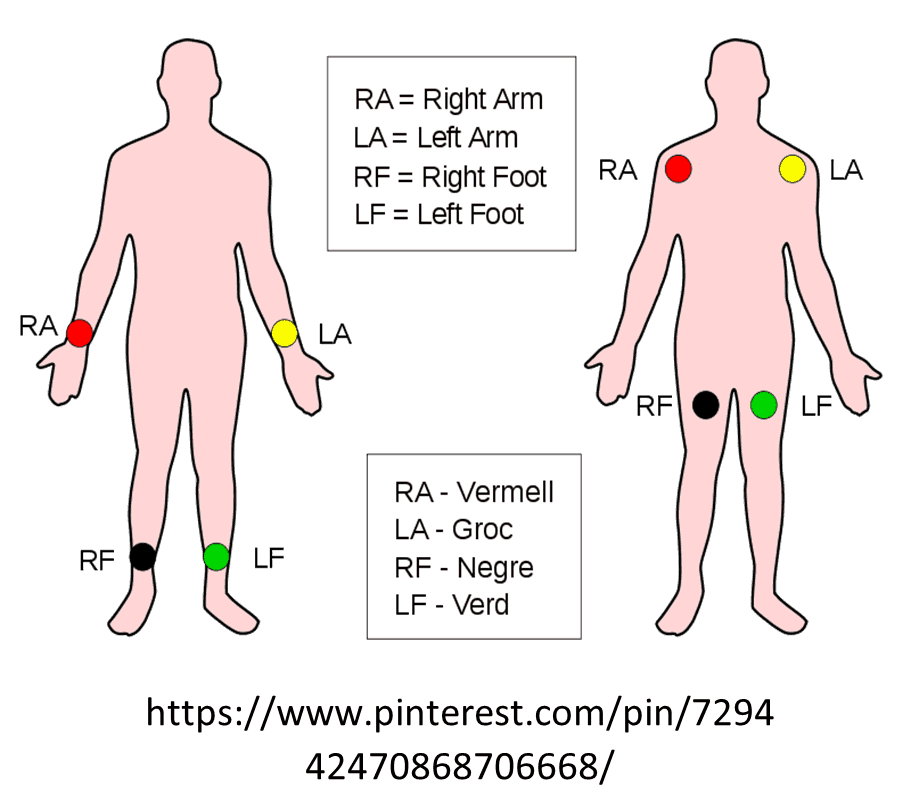
- RA - Right arm or shoulder.
- LA - Left arm or shoulder.
- RL - Right leg or hip.
- LL - Left leg or hip.
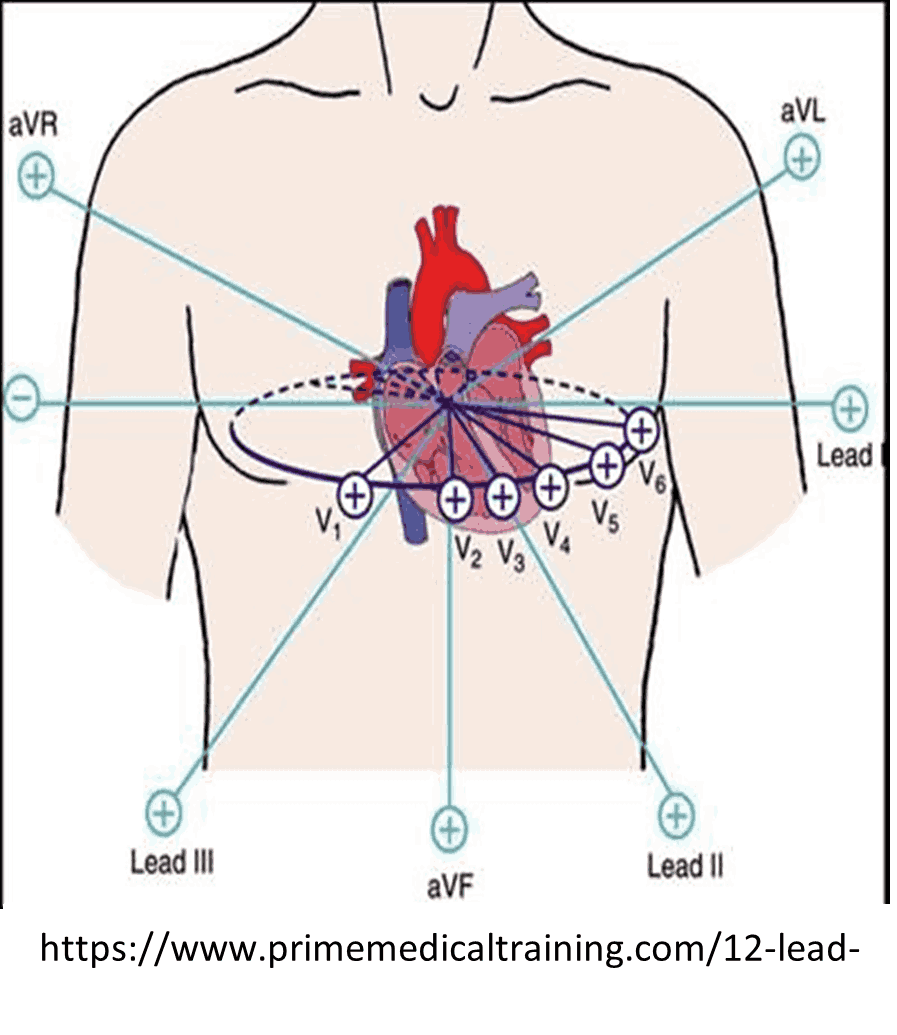
12-lead ECG acquisition, transmission & interpretation in the prehospital environment can be performed only by EMT/AEMT/Paramedics &the reading by AEMT/Paramedics.
STANDING ORDERS:-
Obtain 12-lead ECG with baseline vitals within 10 minutes for potential ACS if available and practical and transmit per local guidelines.
INDICATIONS:-
- Congestive Heart Failure/Pulmonary Edema
- Dysrhythmias, palpitations
- Suspected Acute Coronary Syndrome (chest, jaw, arm, or epigastric discomfort, diaphoresis weakness)
- Syncope
- Shortness of breath
PROCEDURE:-
- Prepare ECG Monitor and connect cable with electrodes.
- Properly position the patient (supine or semi-reclined).
- Enter patient information (e.g. age, gender) into monitor.
- Prep chest as necessary, (e.g. hair removal, skin prep pads).
- Apply chest and extremity leads using recommended landmarks:
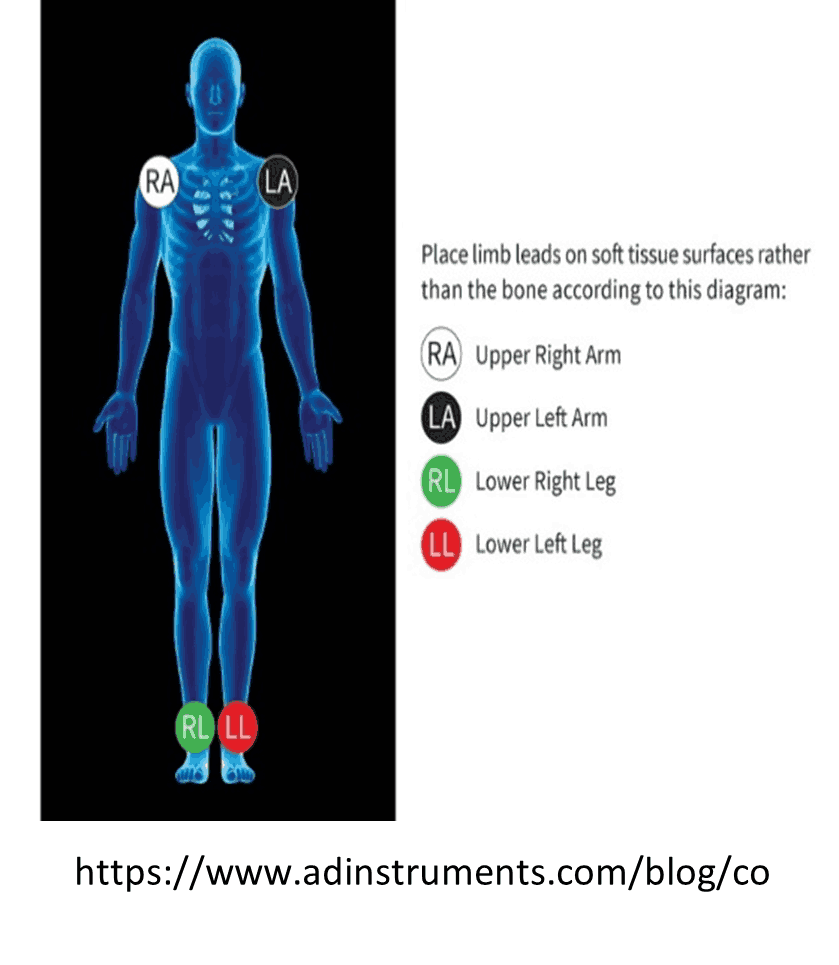
- RA - Right arm or shoulder.
- LA - Left arm or shoulder.
- RL - Right leg or hip.
- LL - Left leg or hip.
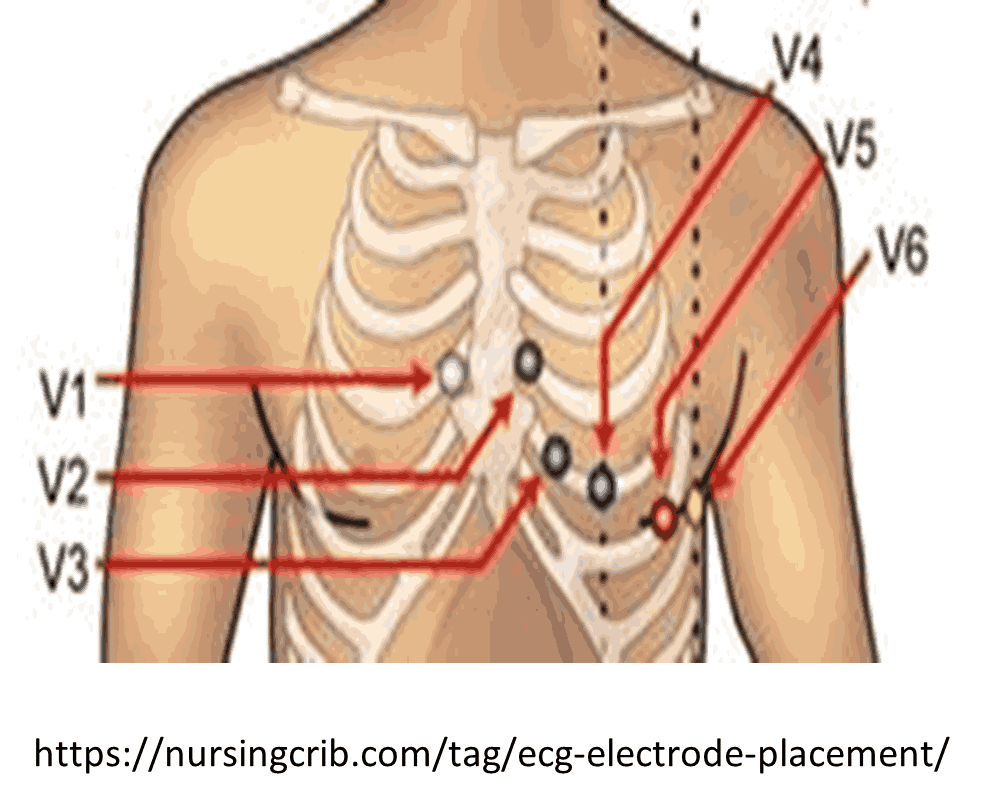
- V1 - 4TH intercostal space at the right sternal border.
- V2 - 4TH intercostal space at the left sternal border.
- V3 - Directly between V2 and V4.
- V4 - 5TH intercostal space midclavicular line.
- V5 - Level with V4 at left anterior axillary line.
- V6 - Level with V5 at left midaxillary line.
- Instruct patient to remain still.
- Obtain the 12-lead ECG, read interpretation, and transmit if possible.
- If the interpretation reads, ***Acute MI*** or ***Acute MI Suspected***, or other similar message, transport patient to the most appropriate.
- facility in accordance with local MI guidelines/agreements and notify receiving facility of a “MI ALERT.”
- If the ECG interprets to be an acute ST-elevation myocardial infarction (MI), transport patient to the most appropriate facility in accordance with local MI guidelines/agreements and notify receiving facility of a “MI ALERT.”
- For patients with continued symptoms consistent with acute coronary syndrome, perform repeat ECGs during transport to evaluate for evolving MI.
- Copies of 12-lead ECG labeled with the patient’s name and date of birth should be left with the receiving hospital and incorporated into the patient’s SIREN record.