Bradycardia - Pediatric
Bradycardia - Pediatric
EMT STANDING ORDERS
- Routine Patient Care.
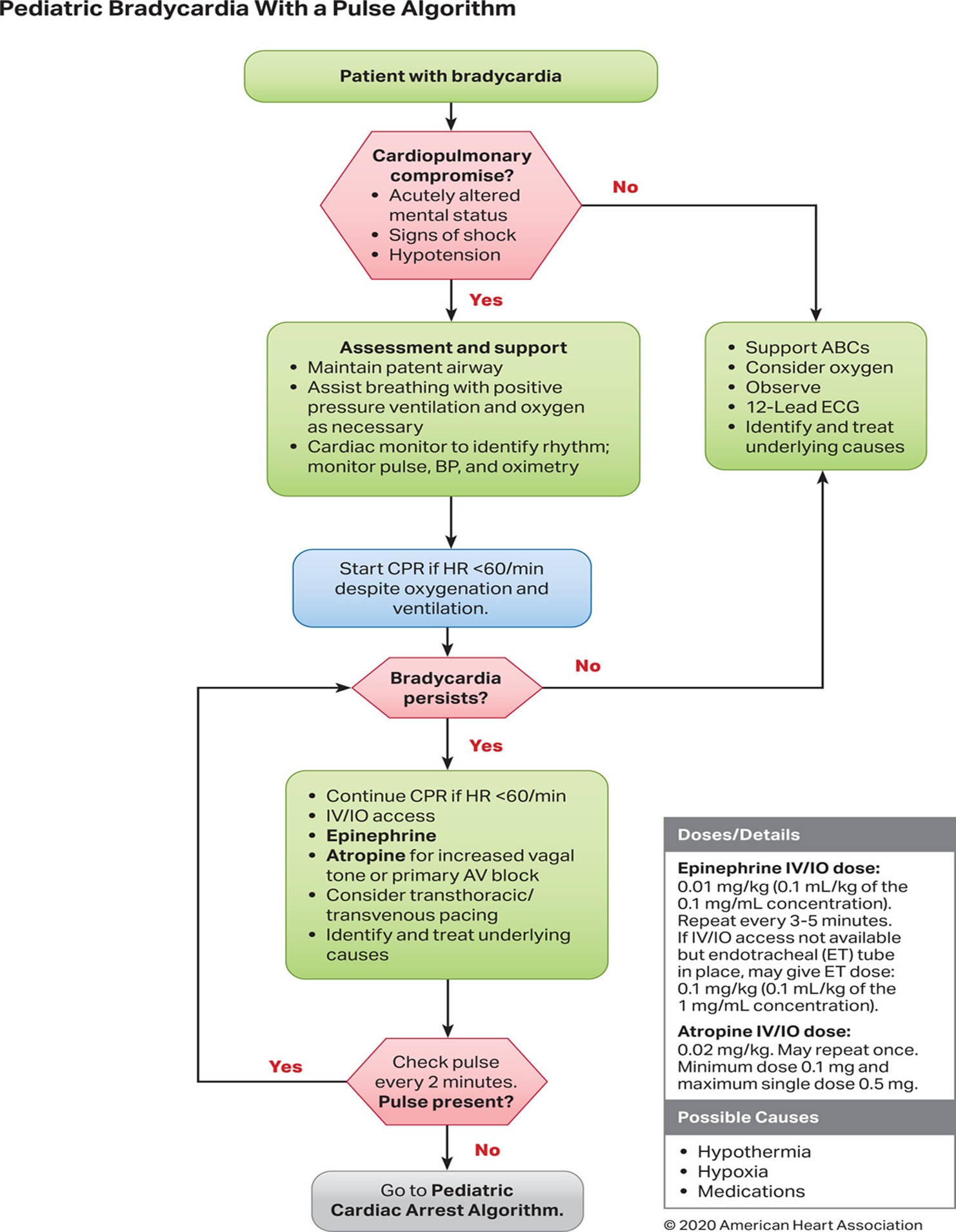
- Consider and treat the underlying causes of bradycardia (e.g., hypoxia, hypoglycemia and hypothermia).
- Begin/ Continue CPR if the heart rate is < 60 bpm AND the child shows signs of poor systemic perfusion with hypo perfusion despite adequate ventilation and oxygenation.
- If serious signs or symptoms (hypotension, acutely altered mental status, signs of shock, ischemic chest discomfort, or acute heart failure); Call for Paramedic intercept, if available.
- Obtain 3 lead ECG if available.
- Establish IV access to KVO.
- Call for AEMT/Paramedic intercept. & Assisst AEMT/Paramedic in patient care.
AEMT/PARAMEDIC STANDING ORDER:
If the patient is hemodynamically unstable:
- Follow PALS guidelines as trained and credentialed
- For Bradycardia with Serious Signs and Symptoms:
- Epinephrine 0.01 mg/kg IV/IO of the (0.1 mL/kg of 0.1mg/ml concentration) every 3 - 5 minutes. If no IV/IO access, may give an ET dose of 0.1 mg/kg (0.1 mL/kg of 1mg/ml concentration).
- Consider atropine 0.02 mg/kg IV/IO for increased vagal tone or AV blocks, may repeat once (maximum single dose 0.5 mg) and (minimum dose 0.1 mg). May give ET dose 0.04-0.06mg/kg.
- Consider transcutaneous pacing. (AS per protocol).
- Identify and treat underlying causes.
- Ask for expert consultation.
Note: Never delay TCP in symptomatic patient while awaiting IV/IO access or atropine.