TRANSCUTANEOS PACING (TCP)
TRANSCUTANEOS PACING (TCP)
OBJECTIVES:-
- Identify patient who will benefit from TCP.
- Identify rhythms, which are best treated by pacing.
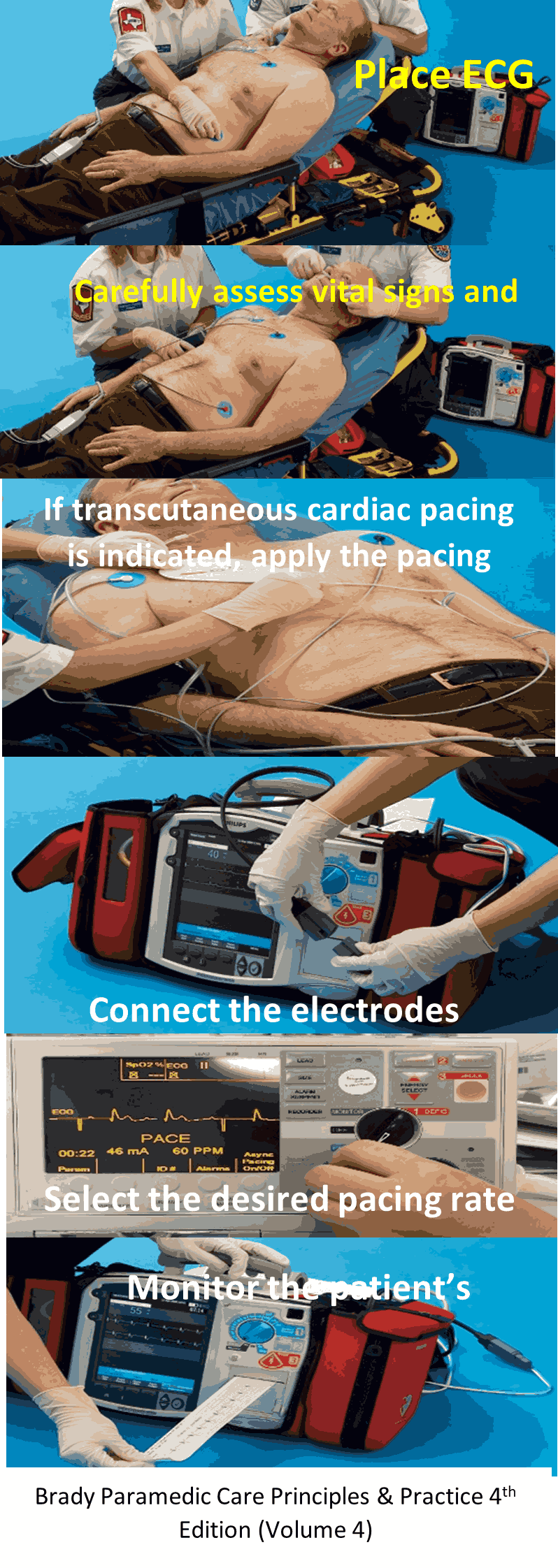
- To deliver an adjustable electrical impulse directly across an intact chest wall for the purpose of rhythmically stimulating the myocardium to increase the mechanical heart rate.
INDICATION OF PROCEDURE:-
- Bradycardia (ECG other than 2nd degree Mobitz type II or 3rd degree AV block).
- 2nd degree Mobitz type II and 3rd degree AV block with a systolic BP < 80 mmHg or 80- 100mmHg with shock like signs or symptoms.
- When cardiac output is compromised due either to the complete failure of cardiac rhythm or to insufficient rate of the patient intrinsic pacemaker.
PROCEDURE
- Undertake universal precautions (BSI).
- Maintain ABC, administer oxygen if needed to maintain O2 Sat >94%.
- Attach Cardiac monitor to analyze rhythm obtain BP and Pulse Oxymetre.
- Establish IV/IO access
- Verify the presence of slow pulse.
- Place patient in supine position away from contact with water and metal.
- Perform patient assessment
- If patient is conscious, explain the procedure.
- Open and inspect the pacing electrodes and insure that the conductive gel is moist.
- Determine the most appropriate and practical electrodes position for the patient, anterior / posterior is preferred.
- Clean the electrode site to insure good adhesion.
- Turn pacing function to “on” position and set the pacemaker rate between 60-80 BPM.
- Set the milli-amperes (mA) to “0” and connect the pacing electrodes to the external pacemaker.
- Increase the mA in an increment of 10 each till you reach 100 then increase it in an increment 5 until electrical capture has occurred (Pacer spike followed by a wide QRS).
- Check patient pulse for mechanical capture, if no pulse carotid and or femoral is palpable for each capture and conducted beat and the patient remain unresponsive to therapy then refer to pulseless electrical activity (PEA) protocol.
MEDICAL DIRECTOR:-
Contact director if
- Capture fails to occur at maximum mA setting (200).
- At any time, a change in rhythm or clinical condition occur.
- In cases where heart rate 60-75 BPM and shock like symptoms persist, pacing may be required
- In the presence of Mobitz II and 3rd degree AV block, atropine administration requires medical consultation.
- Pacing may be required for pediatric patient (40 kg or less) with profound symptomatic bradycardia unresponsive to optimal airway management, oxygenation, epinephrine and atropine
CONTRAINDICATIONS
Patient not meeting blood pressure criteria for application of this protocol.
COMPLICATIONS
- Mild to moderate discomfort (consider morphine 1-2 mg IV/IO or Diazepam 2-10 mg IV/IO).
- Musculoskeletal twitching in upper torso may occur during pacing.