CARDIOVERSION
CARDIOVERSION
OBJECTIVES:-
This is a controlled form of defibrillation for patient who still have organized cardiac activity with a Pulse (supraventricular or ventricular tachydysrhythmias) that result in hemodynamic compromise i.e. Systolic BP less than 80 mmHg with shock like symptoms.
INDICATION OF PROCEDURE:-
- Patient with perfusing ventricular tachycardia.
- Patient with paroxysmal supraventricular tachycardia.
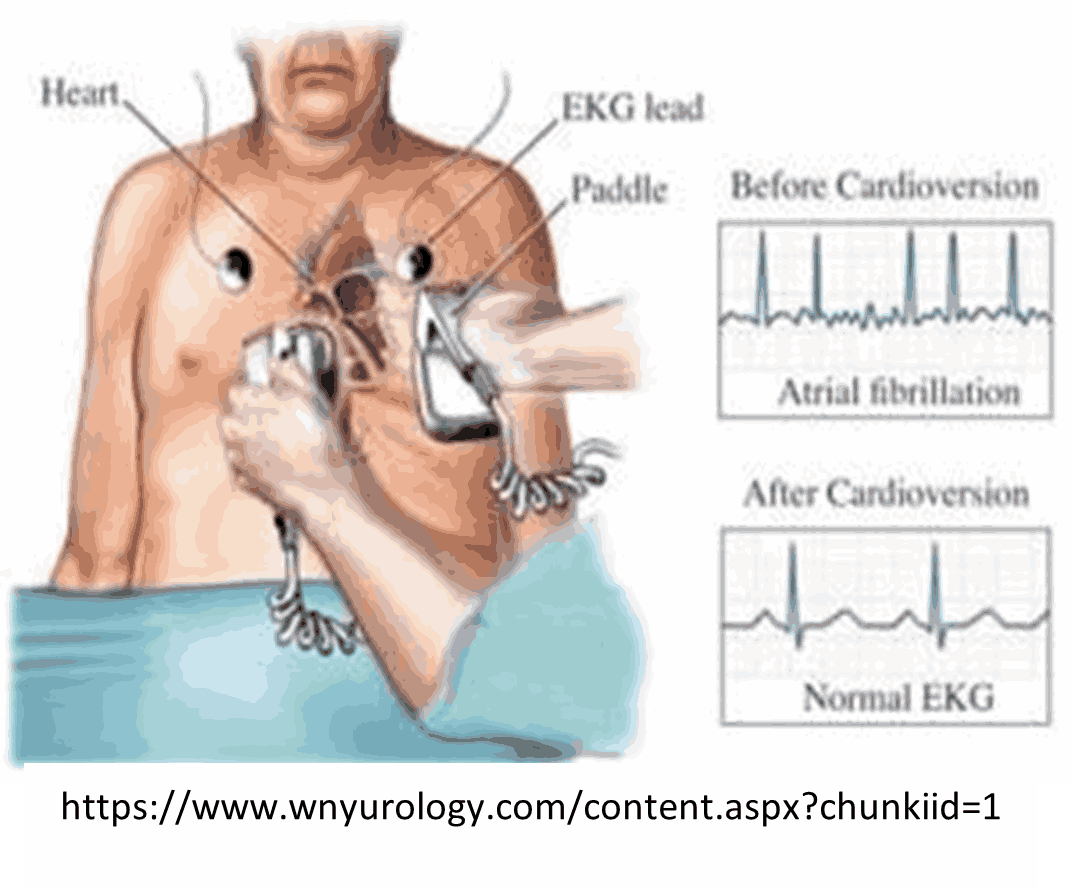
- Rapid atrial fibrillation.
- 2:1 atrial fibrillation.
- Symptomatic patient with hemodynamic instability.
PROCEDURE
- Undertake universal precautions (BSI).
- Maintain ABC
- Attach Monitor to analyze rhythm obtain BP and Pulse Oxymetre.
- Establish IV/IO access
- Verify the absence of pulse and respiration.
- Initiate CPR with C-A-B sequence 5 cycles or 2 minutes (30compressions: 2 breaths)
- Switch the AED ON.
- Place electrodes on the patient chest.
- Connect electrodes to the AED cable.
- Clear the patient to analyze the rhythm.
- If shock is advised.
- Insure all individuals are clear of the patient.
- Deliver shock.
- Immediate resume CPR for 5 cycle 2 minutes without checking for pulse, BVM ventilation and insert oropharyngeal airway.
- After 2 minutes AED will prompt to repeat step G and H by initiate rhythm analysis and deliver additional shocks if advised by the AED.
- If "No shock advised" indicated and the patient remains in cardiac arrest immediately restart CPR beginning with Chest compression.
- Attach patient to manual defibrillator, analyse rhythm and treat according to protocol.
- Transport immediately to hospital while continuing CPR.
PROCEDURE:-
- Take universal precautions.
- Maintain ABC; administer oxygen if needed titrate to maintain O2 Sat <94%.
- Perform patient assessment and take SAMPLE history.
- Place patient in position of comfort away from contact with water and metal.
- Connect to cardiac monitor; to analyze rhythm monitor BP and pulse oximetry
- Confirm supraventricular or ventricular tachydysrthmias.
- Apply electrode gel to the paddles, or place commercial defibrillation pads on the patient thorax.
- Turn on the synchronizer switch (depend on the type of the machine you are using) and charge it to 50-100J initially, verify the machine is detecting the R-waves, if not you may need to reposition the electrodes.
- Make sure nobody is in contact with the patient.
- Press and hold the discharge buttons until the machine discharges on the next R- wave.
- Check pulse and rhythm.
- If there is no change, reset the defibrillator, then cardiovert at 200 joules.
- If there is no change, reset and synchronizer at 200 joules.
- If still no change, reset and cardiovert at 200 joules.
- If the cardiac rhythm converts to a clinically significant dysrthmia, treat it according to specific protocol.
MEDICAL DIRECTOR:
Sedation and analgesia with Valium 5-10 mg IV/IO and morphine 2-5 mg IV/IO may be required prior to Cardioversion.
CONTRAINDICATIONS
Tachydysrthmias due to digitalis toxicity.
COMPLICATIONS
An unsynchronized shock can result in ventricular fibrillation.