Double Sequential
Double Sequential
Defibrillation - Adult
STANDING ORDERS - ADULT
INDICATION:-
Refractory Ventricular Fibrillation / Tachycardia after 5 unsuccessful shocks and a second manual defibrillator is available.
- Recurrent ventricular fibrillation/tachycardia is defined as SUCCESSFULLY CONVERTED by standard defibrillation techniques but subsequently returns. It should NOT be treated by double sequential external defibrillation. It is managed by treatment of correctable causes and use of anti-arrhythmic medications in addition to standard defibrillation
- Refractory ventricular fibrillation/tachycardia is defined as NOT CONVERTED by standard defibrillation. It is initially managed by treating correctable causes and with antiarrhythmic medications. If these methods fail to produce a response, double sequential external defibrillation may be beneficial.
PROCEDURE
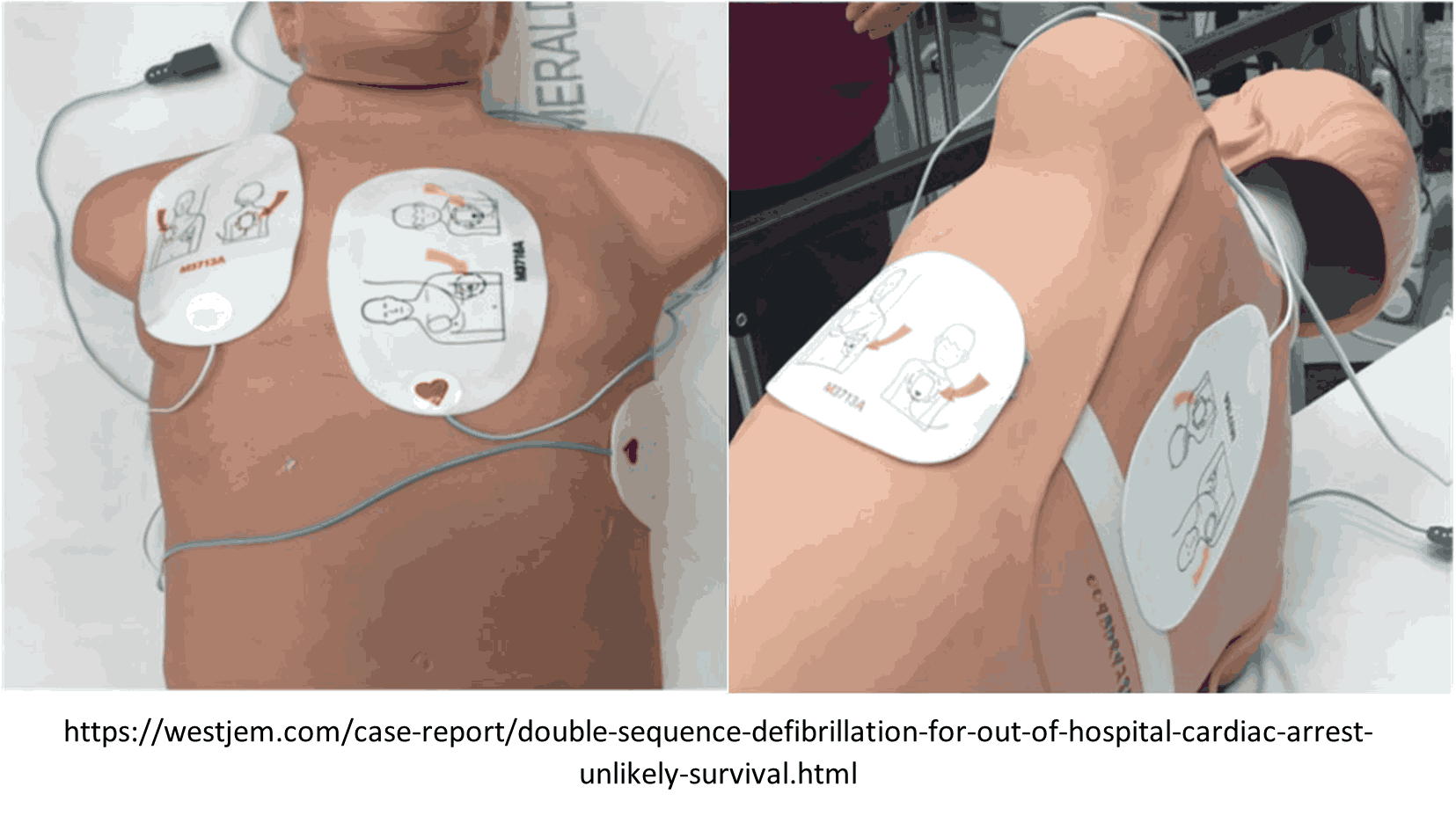
- Prior to attempting Double Sequential Defibrillation, at least one shock should be given using a different vector. Change pad placement from anterior-apex to anterior-posterior.
- Ensure quality CPR and minimally interrupted chest compressions during pad application and procedure.
- Apply a new set of external defibrillation pads adjacent to, but not touching the pad set currently in use.
- Assure that controls for the second manual defibrillator are accessible to the team leader
- Verify that both cardiac manual defibrillators are attached to the patient, that all pads are well adhered, and simultaneously charge both manual defibrillators.
- When both monitors are charged to maximum energy settings and all persons are clear, push both shock buttons as synchronously as possible.
- May repeat procedure every 2 minutes as indicated if refractory ventricular fibrillation/tachycardia persists.
PEARLS:-
- Continue compressions when defibrillators are charging.
- During interruptions compressor’s hands should hover over the chest.
- Pre-charge manual defibrillators prior to rhythm check to ensure rapid defibrillation if a shockable rhythm is present. If no shock is indicated, disarm the device (dump e charge).
- Depending on your local hospital resources, some refractory ventricular fibrillation patients may benefit from emergent cardiac catheterization. For this small patient population, transportation (ideally with a mechanical CPR device) may be indicated. Transporting these patients directly to the Cath lab should be done in collaboration with online Medical Direction and interventional cardiology.
- Caution: There are case reports of monitors being damaged by this procedure.