INTRAOSSEOUS INFUSION (IO)
INTRAOSSEOUS INFUSION (IO)
DEFINITION:-
Intraosseous insertion establishes access in a critically ill patient where venous access cannot be rapidly obtained. The bone marrow space serves as a noncollapsible vein” and provides access to the general circulation for the administration of fluids and resuscitation drugs. This protocol applies to all appropriate IO insertion sites.
OBJECTIVES
- Gain emergent vascular access in the absence of peripheral venous access.
- Select appropriate anatomical location for insertion of needle (proximal tibia).
- Identify indications /contraindications for procedure.
- Use proper technique for insertion /infusion.
- Properly secure and frequently monitor the needle and site.

INDICATION
- Any life threatening illness or injury requiring immediate pharmacological or volume intervention.
- Two IO attempts may be made one in each proximal tibia.
- Drug or fluid resuscitation of a patient in profound hypovolemia shock or other critical illness and in need of immediate life-saving intervention and unable to rapidly obtain peripheral IV access.
- If IV access cannot be obtained or following two unsuccessful peripheral IV attempts, IO access may be used as a vascular device in cardiac arrest.
- In cardiac arrest, proximal humeral is preferred over anterior tibial in adults.
CONTRAINDICATIONS.
- Placement at an infected site.
- Placement at site where IO was already attempted.
- Conscious patient with stable vital signs.
- Peripheral vascular access readily available.
- Placement in or distal to a fractured bone. Or Suspected or known fracture in the extremity targeted for IO infusion, but fracture of the femur is a relative contraindication.
- Patient with documented bone disorders.
- Previous attempts in the same bone.
- Cellulitis at the intended site of the procedure.
COMPLICATIONS:-
- Infusion rate may not be adequate for resuscitation of ongoing hemorrhage or severe shock, extravasation of fluid, fat embolism, and osteomyelitis (rare).
- Infection.
- Extravasations of fluids.
- Fat emboli.
- Compartment syndrome.
EQUIPMENT
- 15 - 19-gauge bone marrow needle or approved intraosseous infusion device.
- Gloves and povidone-iodine, chlorhexidine solution or alcohol wipes.
- Primed IV tubing, IV stopcock.
- 10 mL syringe with 0.9% NaCl.
- Pressure pump / bag or 60 mL syringe for volume infusion or slow push.
- Paramedic only: 1 vial of 2% lidocaine (preservative free).
- 5 mL syringe.
PROCEDURE
- Undertake universal precautions.
- Perform patient assessment, mechanism of injury.
- Place patient in position of comfort, if trauma patient keeps head and neck in neutral position.
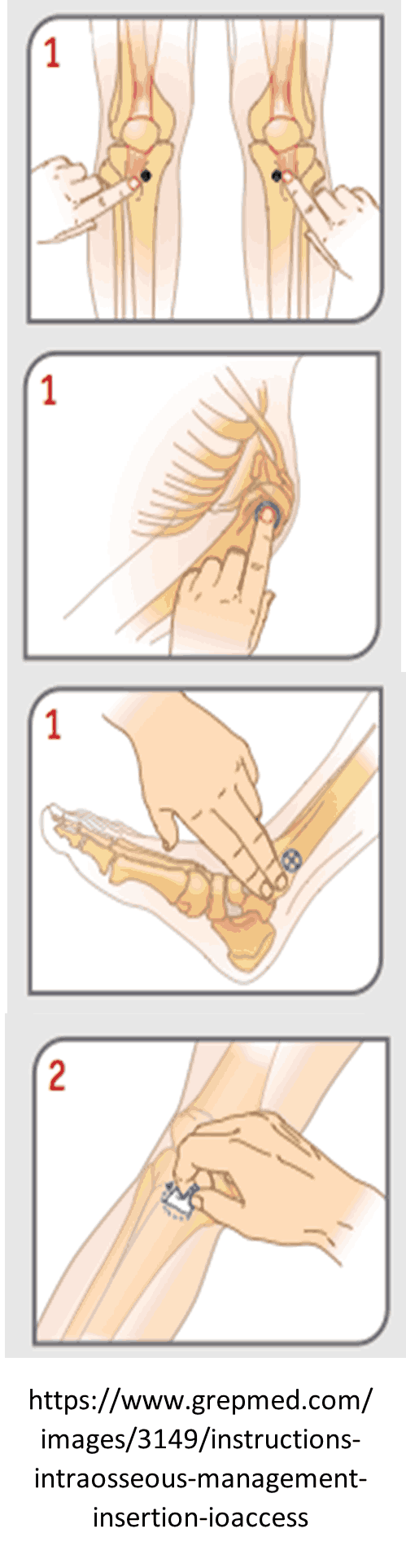
- Identify the bony landmarks as appropriate for device, the site of choice is:
- Anterior tibia, one finger width below the tubercle/or just
- proximal to medial malleolus of the distal tibia.
- Distal Femur
- Medial malleolus
- Anterior-superior iliac spine.
- Choose correct needle size: 45 mm proximal humerus, 25 mm anterior tibial, 15 mm anterior tibial skin and bone (thin). Prep the site. Scrub site with alcohol wipe or other cleaning solution and cleanse the skin allow to dry.
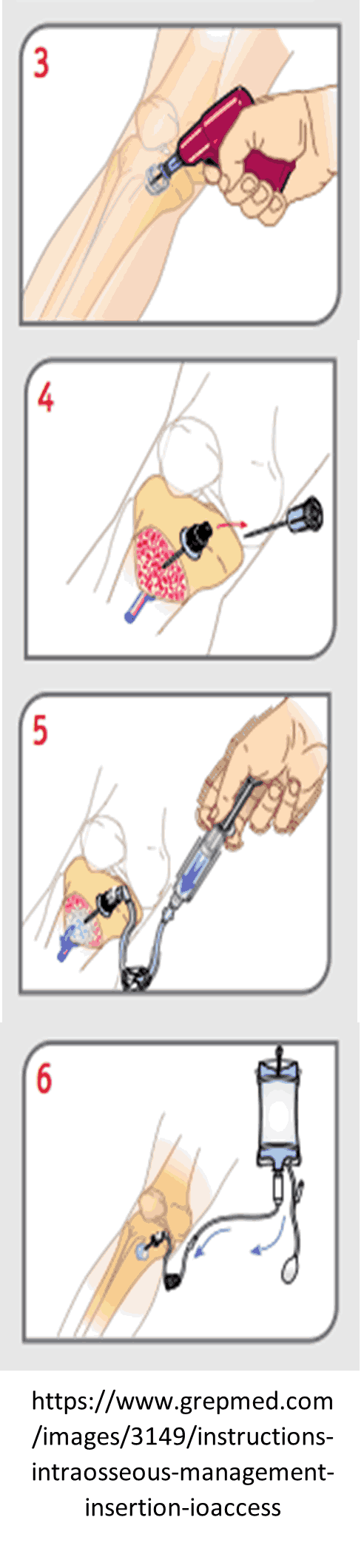
- Insert the needle at 60-90-degree angle to the skin with the point directed towards the foot, use-screwing motion until penetration into the marrow is achieved as noted by decreased resistance.
- Remove the stylet and return it to the sterile field.
- Needle is appropriately placed if the following are present:
- Attempts to aspirate marrow into 10 ml syringe filled with 5 ml. of normal saline If appropriate, aspiration of blood with marrow particulate matter will show in the syringe. (aspiration of bone marrow is not always possible)
- Infuse 5ml of saline from a 10 ml syringe to check placement and to flush the needle of any clots. Infusion of saline does not result in infiltration at the site.
- If marrow cannot be aspirated but saline can be infused easily and there is no evidence of swelling around the site, it is assumed that the needle has been properly placed.
- Needle stands without support.
- Attach IV tubing, with or without stopcock.
- Stabilize the needle:-
- Consider utilizing an available stabilization device as recommended by the manufacturer
- Stabilize needle on both sides with sterile gauze and secure with tape (avoid tension on needle).
- Attach the appropriate infusion set (fluids will need to be placed under pressure to overcome the resistance, gravity alone is usually insufficient).
- Apply ID bracelet to indicate patient has had an IO placed or attempted.
- Prior to IO syringe bolus (flush) or continuous infusion in alert patients:
- Ensure that the patient has no allergies or sensitivity to lidocaine.
- SLOWLY administer lidocaine 2% (preservative free) through the IO device catheter.
- Allow 2 - 5 minutes for anesthetic effects, if possible:
- Adult: 20 - 50 mg (1 - 2.5 mL) 2% lidocaine.
- Pediatric: 0.5 mg/kg 2% lidocaine (maximum 50 mg).
- Flush with 10 mL of 0.9% NaCl rapid bolus x 3 prior to use
- Recommend use of a stop cock inline with syringe for bolus infusions.
- Use a pressure bag for continuous 0.9% NaCl infusions.
MEDICAL DIRECTOR:-
- IO attempt on a pediatric patient who does not meet the above criteria e.g. severe burn, seizures…etc.
- For more than 2 attempts of IO.
PEARLS:- Any fluid or medication that can be administered through an IV may be administered through an appropriately-placed IO device. May only attempt one IO needle per site. Notify ED of missed sites.IO access is not indicated simply for inability to start an IV, but rather is reserved for patients with profound shock or other critical illness.