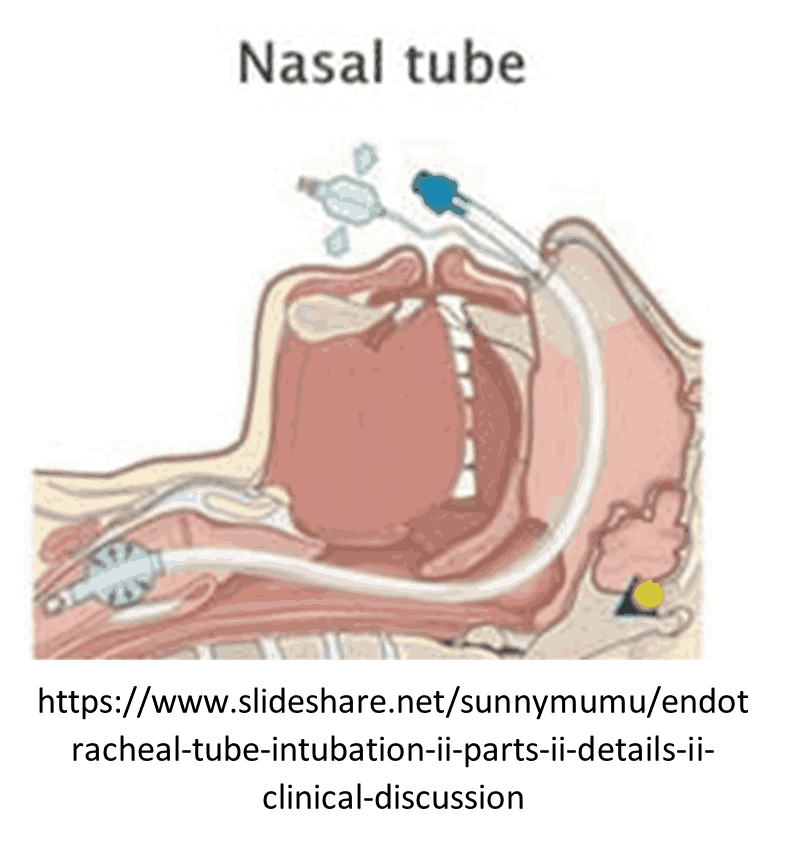
Nasotracheal Intubation
Nasotracheal Intubation
ARAMEDIC STANDING ORDERS - ADULT
INDICATIONS
Impending respiratory failure with intact gag reflex, or jaw is clenched and unable to be opened in spontaneously breathing patient
CONTRAINDICATIONS:
- Apnea.
- Nasal obstruction.
- Suspected basilar skull fracture.
- Severe facial trauma or suspected facial fractures.
- Patient fits on a pediatric length-based resuscitation tape.
PROCEDURE:
- Pre-medicate nasal mucosa with 2% lidocaine jelly and vasoconstricting nasal decongestant spray such as neo-synephrine, if available.
- Pre-oxygenate the patient.
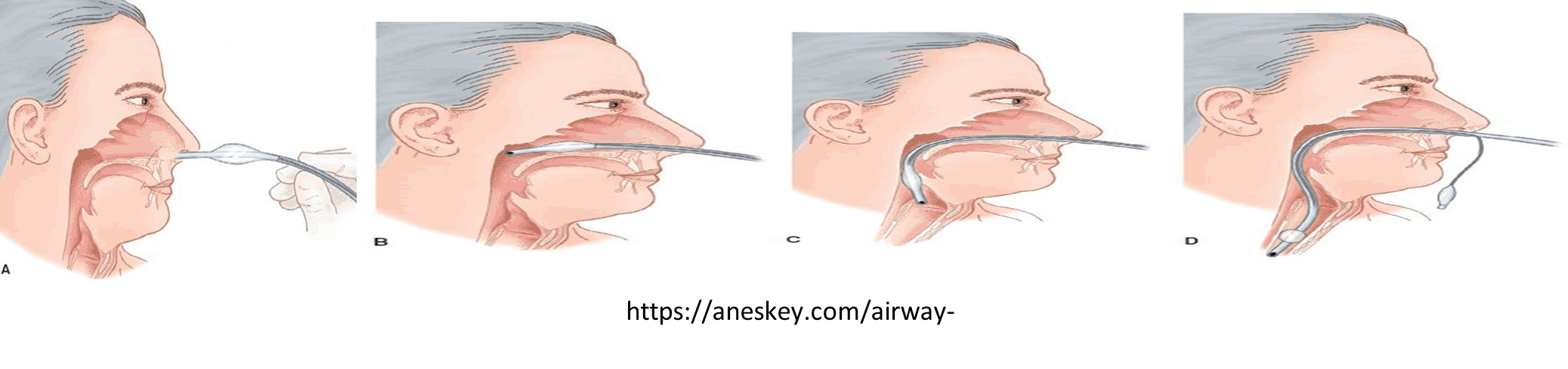
- Select the larger and less obstructed nostril and insert a lubricated nasal airway.
- Lubricate the ETT with water-based lubricant.
- Remove the nasal airway and gently insert the ETT with continuous waveform capnography monitoring, keeping the bevel toward the septum (a gentle rotation movement may be necessary at the turbinates).
- Continue to advance the ETT while listening for maximum air movement and watching for capnography waveform.
- At the point of maximum air movement, indicating proximity to the level of the glottis, gently and evenly
advance the tube through the glottic opening on inspiration.
- If resistance is encountered, the tube may have become lodged into the pyriform sinus and you may note tenting of the skin on either side of the thyroid cartilage
- If this happens, slightly withdraw the ETT and rotate it toward the midline and attempt to advance the tube again with the next inspiration.
- Upon entering the trachea, the tube may cause the patient to cough, buck, strain, or gag. This is normal. Do not remove the ETT. Be prepared to control the cervical spine and be alert for vomiting.
- Placement depth should be from the nares to the tip of the tube: approximately 28 cm in males and 26 cm in females.
- Inflate cuff with 5 - 10 mL of air.
- Confirm appropriate placement by waveform capnography, symmetrical chest-wall rise, auscultation of equal breath sounds over the chest, a lack of epigastric sounds with bagging.
- Secure the ETT, consider applying a cervical-collar and securing patient to a long back backboard (even for the medical patient) to protect the placement of the ETT.
- Ongoing monitoring of ETT placement and ventilation status using waveform capnography is required for all patients.
- Document each attempt as a separate procedure in SIREN. An attempt is defined as placement of the tube into the patient’s nostril. For each attempt, document the time, provider, placement success, pre-oxygenation, ETT size, placement depth, placement landmark (e.g. cm at the naris), and confirmation of tube placement including chest rise, bilateral, equal breath sounds, absence of epigastric sounds and end-tidal CO2 readings.
Sedation is not usually necessary following nasotracheal intubation.
- Fentanyl 50 — 100 mcg slow IV/IO push. May repeat every 15 minutes as needed for anesthesia (maximum 300 mcg). AND
- Midazolam 2.5 —5 mg IV/IO every 5 — 10 minutes as needed for sedation (maximum 20 mg) OR
- Lorazepam 1 — 2 mg IV/IO every 15 minutes as needed (maximum 10 mg).
Contact Medical Direction for additional dosing.