NEEDLE CRICOTHYROIDOTOMY
NEEDLE CRICOTHYROIDOTOMY
(TRANSTRACHEAL JET INSUFFLATION)
The Objectives:
- Identify patient with a compromised airway, who will require the insertion of needle Cricothyroidotomy.
- Provide the necessary and appropriate equipment and personnel.
- Confirm proper needle placement, maintain and continuously monitor needle placement and patient condition.
INDICATIONS
- Severe laryngeal odema,
- Trauma to face and upper airway or upper airway obstruction etc. which prohibits the placement of endotracheal tube airway,
- Cannot be relieved by using a laryngoscope and Magill forceps, and
- Cannot be managed by BVM with an oropharyngeal airway.
The following procedure is an effort to maintain awareness of a procedure that occurs rarely in the EMS system. Ultimately, this procedure should be practiced on a regular basis to maintain proficiency.
PLEASE NOTE: This procedure describes a generally acceptable open cricothyrotomy and will differ from services that employ percutaneous kits. The inclusion of this procedure.
DOES NOT mandate that all providers use this exact procedural description. Providers should employ the procedure they are trained, practiced and most comfortable with. This procedure is one of multiple acceptable means to perform this procedure. Regardless of the procedure type, it is essential that CDAA paramedics are familiar with the available supplies and materials.
The primary indication for surgical cricothyrotomy is failure to maintain the airway (including oxygenation, ventilation, and protection) through other less invasive means in a patient 8 years or older with palpable landmarks. This has occurred predominantly in trauma cases with disruption of the face and normal airway anatomy and in choking patients. Even in some dramatic facial injuries, the airway may be adequately managed by sitting the patient up and leaning forward, as long as the other injuries allow.
MATERIALS/EQUIPMENT
- Cuffed tracheostomy tube or 6.0 - 7.0 ETT
- Tracheal hook or bougie
- Trousseau dilator (if available).
- Syringe to inflate the cuff
- Scalpel.
- Swabs/skin prep.
PROCEDURE
Only needle Cricothyroidotomy should be performed for patients less than 10 years of age who require Cricothyroidotomy (surgical Cricothyroidotomy contraindicated).
- Undertake universal precautions.
- Maintain ABC
- Maintain Oxygenation > 94%
- Attach a Cardiac monitor to analyze rhythm, and obtain BP and Pulse Oxymeter (SaO2).
- Establish IV/IO access
- Identify a patient who will require needle Cricothyroidotomy.
- Place the patient in supine position, if trauma patient stabilizes neck and spine (keep in neutral position).
- Perform patient assessment, mechanism of injury.
- Assemble and prepare all equipment necessary for procedure.
- Connect to cardiac monitor, pulse oximetry, and blood pressure cuff.
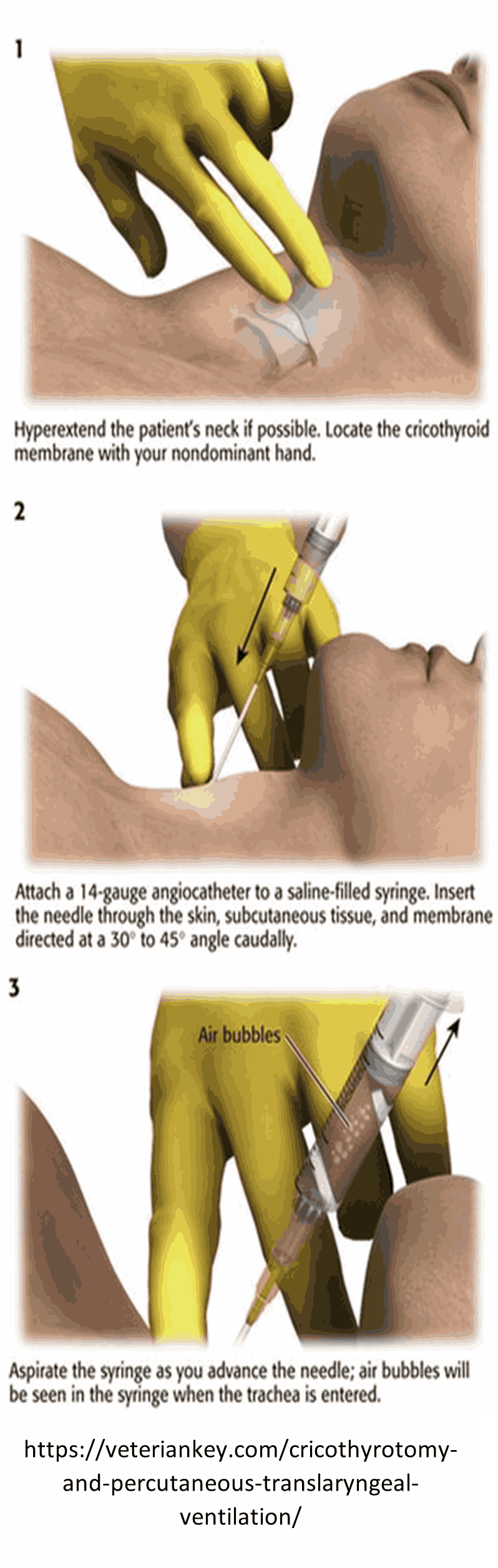
- Extend the neck when possible to ensure best access to the trachea. Swab/cleanse the area.
- Immobilize the trachea with your non-dominant thumb and middle finger while palpating the cricothyroid membrane with
your non-dominant index finger.
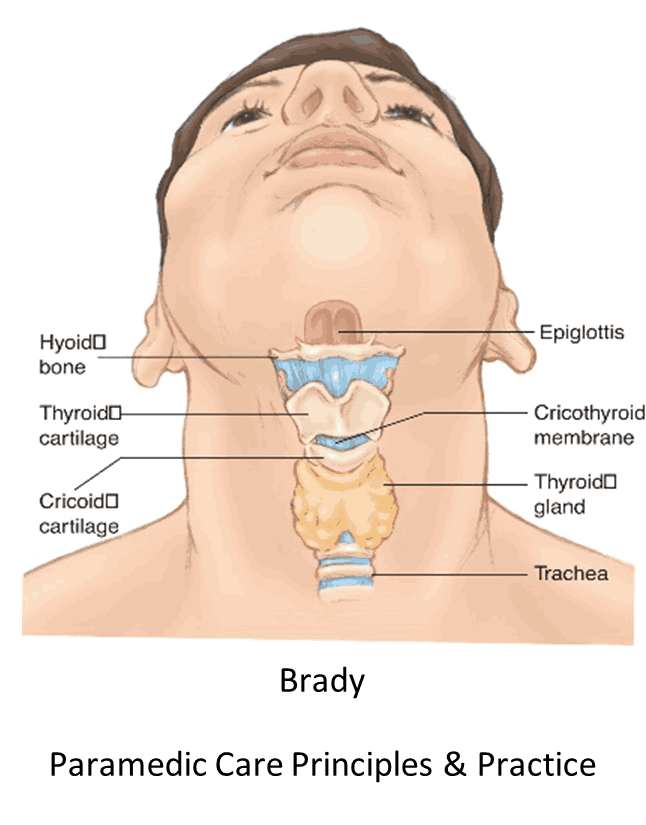
Note: The cricothyroid membrane is immediately BELOW the thyroid cartilage.
- Make a 3 - 5 cm vertical incision over the cricothyroid membrane through the skin and subcutaneous tissues.
Note: Severe bleeding is possible with this procedure and may occur at this or the following steps. Be prepared to suction and provide direct pressure to control bleeding.
- Palpate the membrane through the incision to confirm anatomy.
- Make a small (1 cm or less) incision horizontally through the cricothyroid membrane.
- Insert 14-16 gauges (Adult) and 18-20 gauges (Pediatrics) over the needle catheter through the cricothyroid membrane at 45-degree angle toward the feet. Or Insert the tracheal hook or bougie in the opening of the membrane and rotate toward the head while maintaining hold of the thyroid cartilage with your non-dominant hand.
- If Trousseau dilator available, insert into the incision site and spread vertical then rotate 90 degrees until the dilator is parallel with the neck.
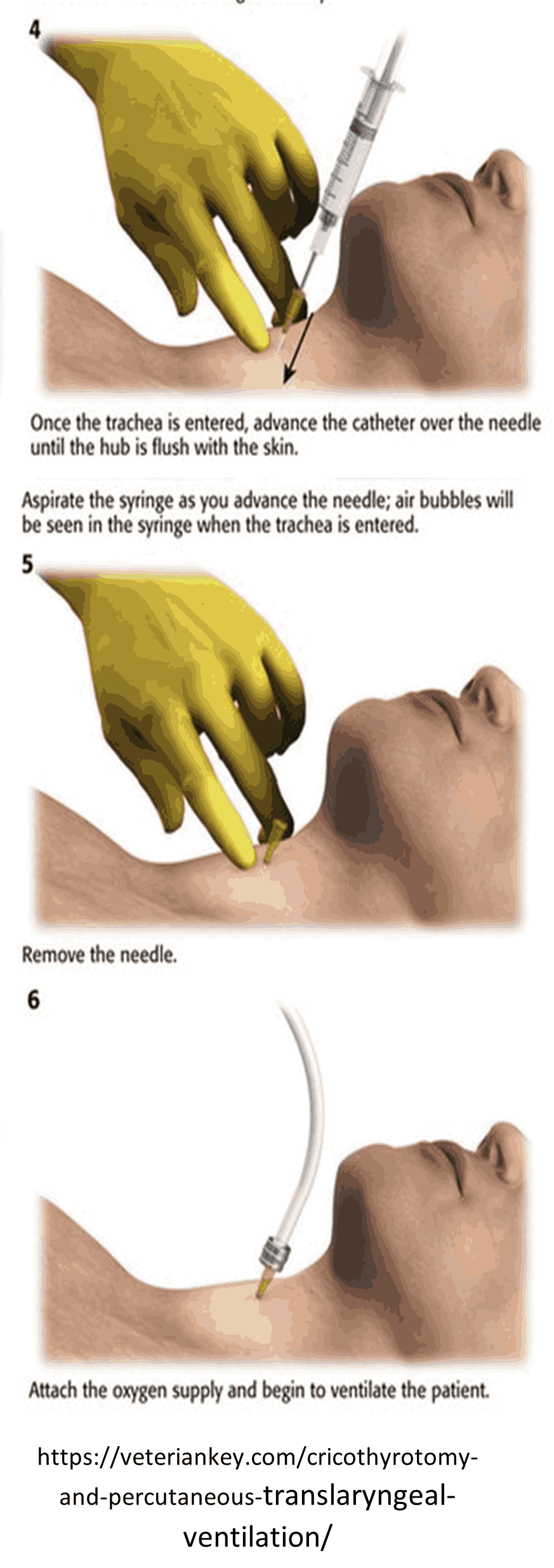
- Insert the cuffed tracheostomy tube or ETT tube into the incision site. Advance until the flanges rest on the skin of the neck (when using tracheostomy tube).
- Carefully remove the dilator (if used), tracheal hook and obturator of the tracheostomy tube.
- Inflate the balloon of the tracheostomy tube/ETT.
- Ventilate and confirm position by physical exam and ETCO.
- Aspiration of air with a syringe indicates tracheal entry or feeling of POP or not to exceed 1 cm in depth as the needle penetrates the membrane.
- Hold needle in place and advance catheter, then remove needle.
- Attach catheter hub to intermittent jet oxygen insufflator valve.
- Confirm tube placement by equal chest rise, lung auscultation and absences of epigestric sounds.
- Secure the tube in place.
- Dress incision site.