Percutaneous Cricothyrotomy
Percutaneous Cricothyrotomy
AEMT/PARAMEDIC STANDING ORDERS
INDICATIONS:
- Failed airway: A patient whose airway cannot be successfully managed by any other means.
- All other methods have been exhausted including BVM, blind airway device, and intubation attempts;
- Massive mid-face trauma precluding use of BVM, obstruction, trismus (clenching).
- Inability to control the airway using less invasive measures.
- Last Resort: All other airway management techniques have failed. Unable to ventilate or oxygenate the patient.
PROCEDURE
- Can use Rusch QuickTrach or other approved device. Choose an appropriate sized device.
- Pre-oxygenate patient when possible.
- Assemble all available additional personnel.
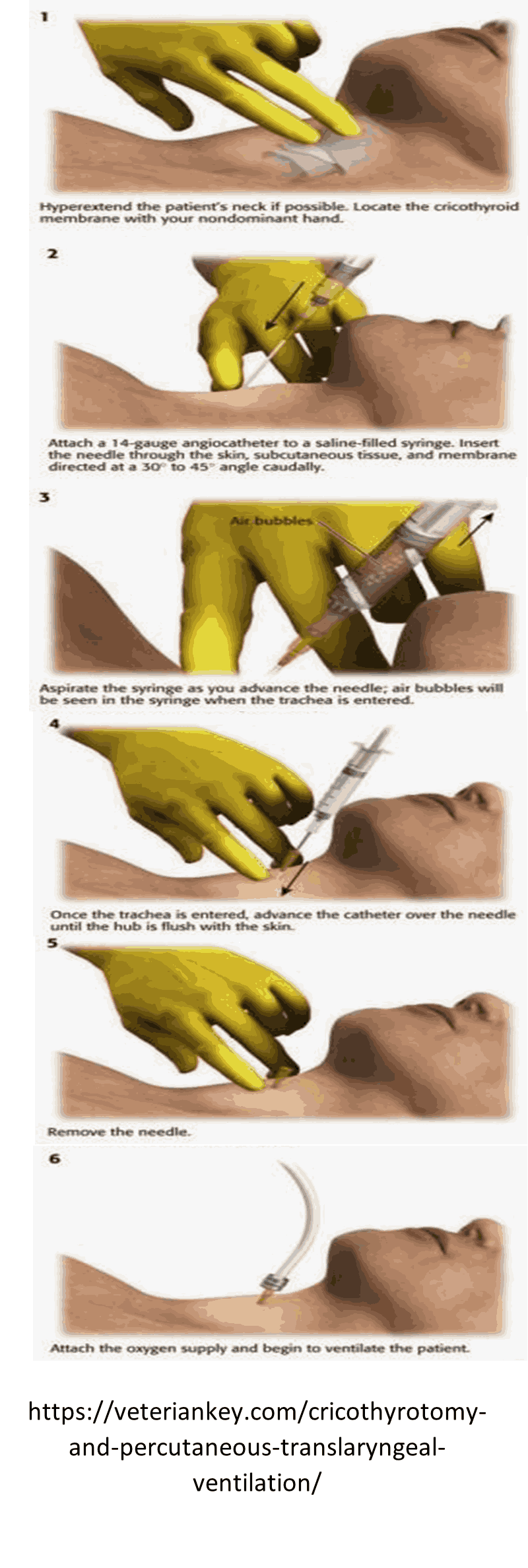
- Locate the cricothyroid membrane at the inferior portion of the thyroid cartilage (with head in neutral position, the membrane is approximately 3 finger widths above the sternal notch). May be difficult to locate in obese patients.
- Hold skin taut over the membrane and locate the midline.
- Prep area, preferably with betadine.
- Hold the needle bevel up at a 90 degree angle, aimed inferiorly as you approach the skin.
- Puncture the skin with the needle and continue with firm, steady pressure while aspirating for air with the syringe.
- As soon as air is aspirated freely, stop advancing the needle/airway assembly.
- Modify the angle to 60 degrees from the head and advance to level of the stopper.
- Remove the stopper while holding the needle/airway assembly firmly in place.
- Do not advance the needle further.
- Hold the needle and syringe firmly and slide only the plastic cannula along the needle into the trachea until the flange rests on the neck. Carefully remove the needle and syringe.
- Secure the cannula with the neck strap.
- Apply the EtCO2 detector.
- Confirm placement with the use of breath sounds, pulse ox, EtCO2 and waveform capnography.
- Ensure 100% FiO2 to BVM via supplemental 02
NOTE: if the patient is obese and no air can be aspirated with the stopper in place, you may remove the stopper and continue advancing until air is aspirated. Be aware that without the stopper risk of perforating the posterior aspect of the trachea is greatly increased.).