Routine Patient Care for (EMTAEMTP)
RESPOND TO SCENE IN A SAFE MANNER
- Review dispatch information.
- Use Incident Command System (ICS) for all responses and scene management.
SCENE ARRIVAL AND SIZE-UP
- Standard precautions, scene safety, environmental hazards assessment, number of patients, need for additional resources, and bystander safety.
- Initiate Mass Casualty Incident (MCI) procedures as necessary.
- Call for AEMT/Paramedic intercept, if needed, for patients with unstable vital signs, respiratory distress or other life-threatening conditions.
PATIENT APPROACH
- Determine mechanism of injury / nature of illness.
- If patient is in cardiac arrest, refer to the Cardiac Arrest Protocol - Adult (1 Cardiac) & Pediatric (4 Cardiac).
- Place the Patient in Supine Position or Position of comfort.
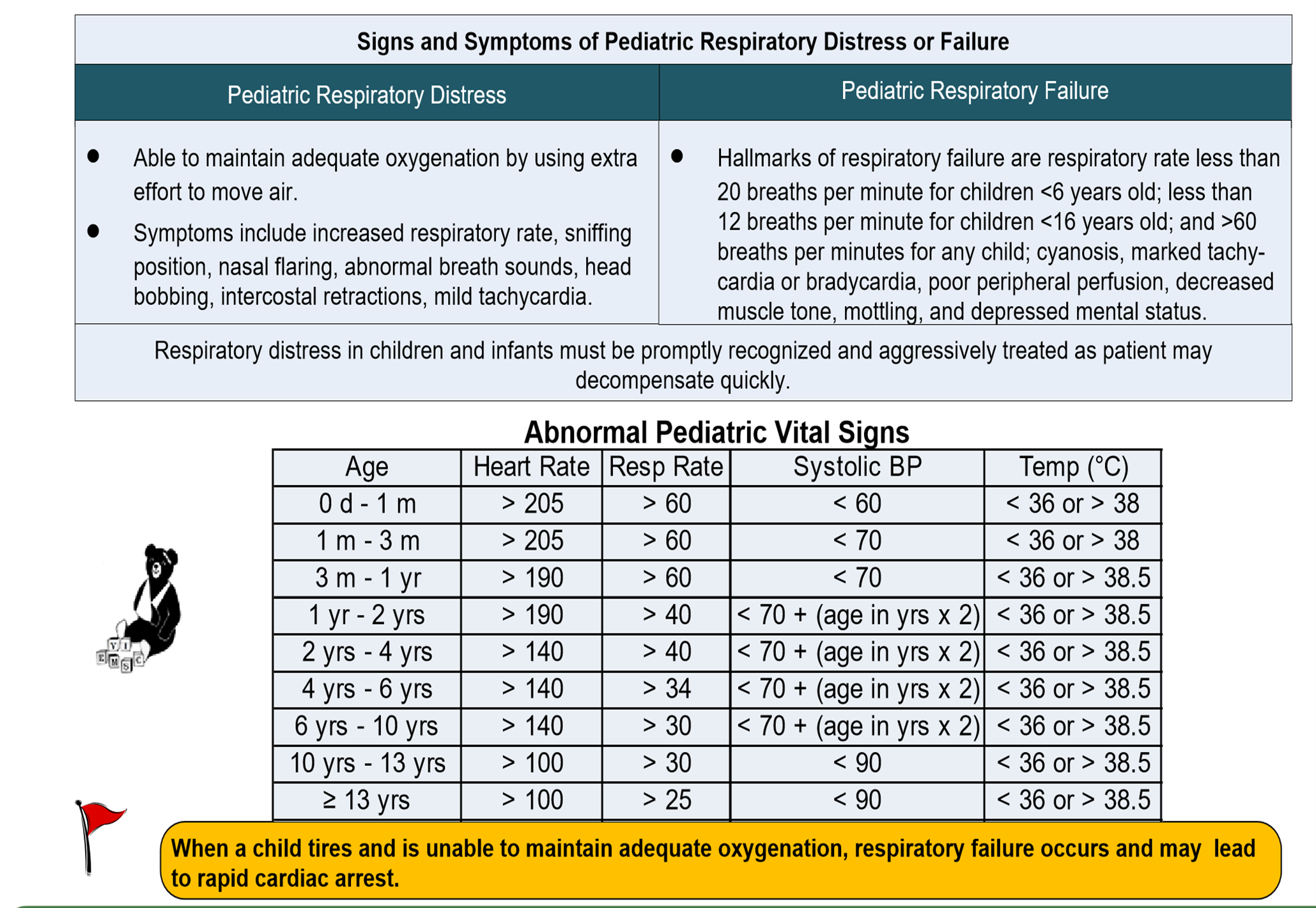
- Determine if pediatric protocols apply.
“Pediatric Patient” is defined as a child
who aged below 12yeas of age or fits on a length- based resuscitation tape up
to 36 kg (79 lbs) or 145 cm (57 in). CDAA EMS Protocol strongly encourages the use
of a pediatric reference system when treating pediatric patients. Stations
should adopt and train with a system that uses weight, length, or age to identify
normal ranges of vital signs and appropriate equipment sizes. The system should also
identify pediatric medication doses by volume and minimize the need for medication
Contact Medical Direction in case any uncertainty exists regarding drug
dosing.
- Establish responsiveness.
- General impression.

| Pediatric Assessment Triangle. | |||
| Appearance | Work of Breathing | Circulation to Skin | |
| Pediatric | Muscle tone, Instructiveness, consolability, Gaze/Look, speech/Cry | Airway Sounds, Body Position, Head bobbing, Chest Wall Retractions, Nasal Flaring, Grunting | Pallor, Mottling, Cyanosis |
Determine if DNR protocol applies.
Primary Assessment
AIRWAY AND BREATHING
- Assess the patient for a patent Airway. If the airway is not patent, take immediate action to correct it (Open & Re Open).
- Assess Breathing:
Breathing Present Yes No Speed Normal Slow Fast Regularity Regular Irregular
- Rate, Effort, Tidal volume, and Breath Sounds.
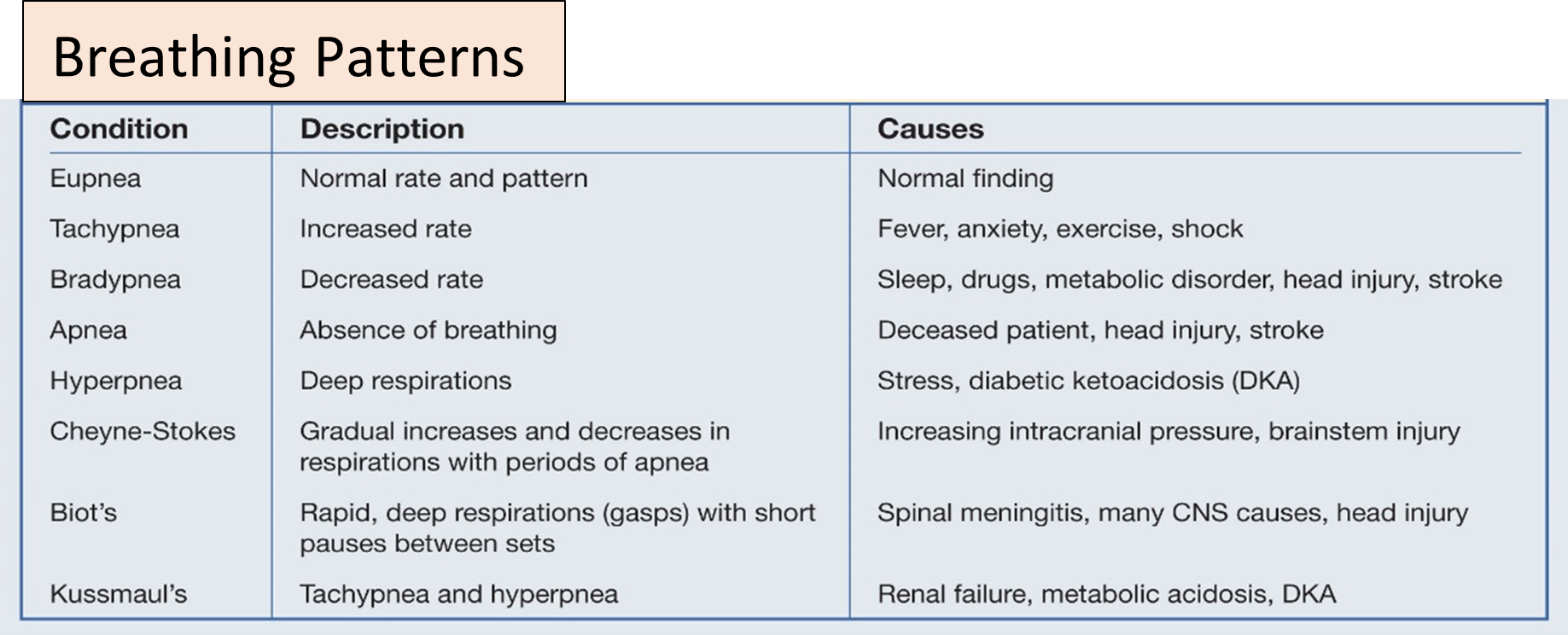
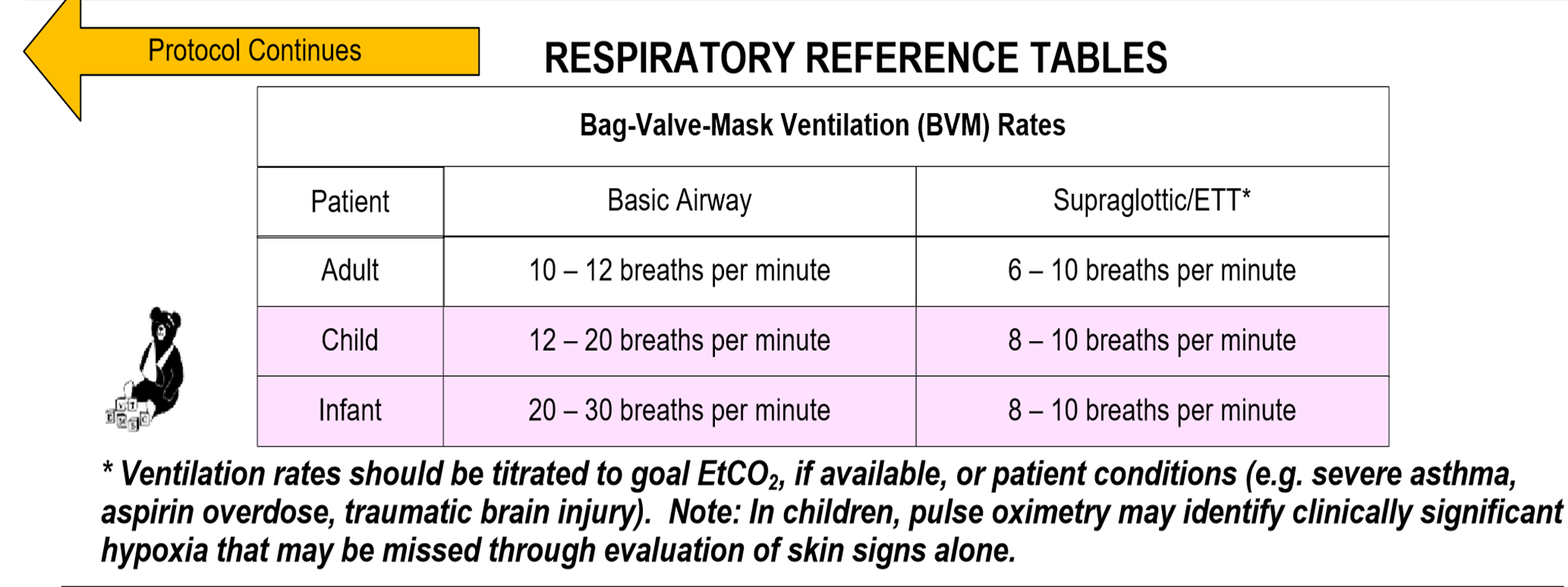
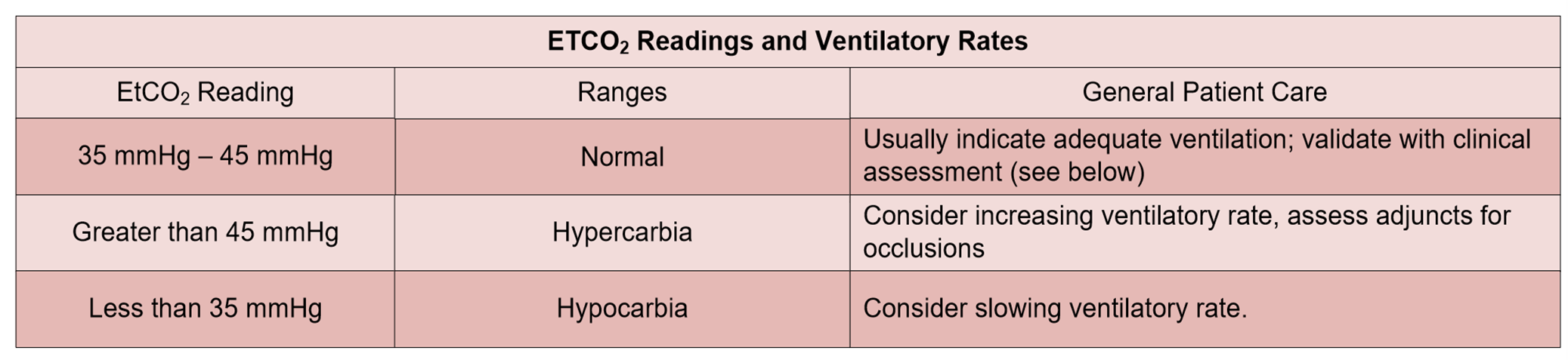
- If breathing is inadequate (slow, shallow), ventilate with 100% oxygen using bag-valve-mask (BVM).
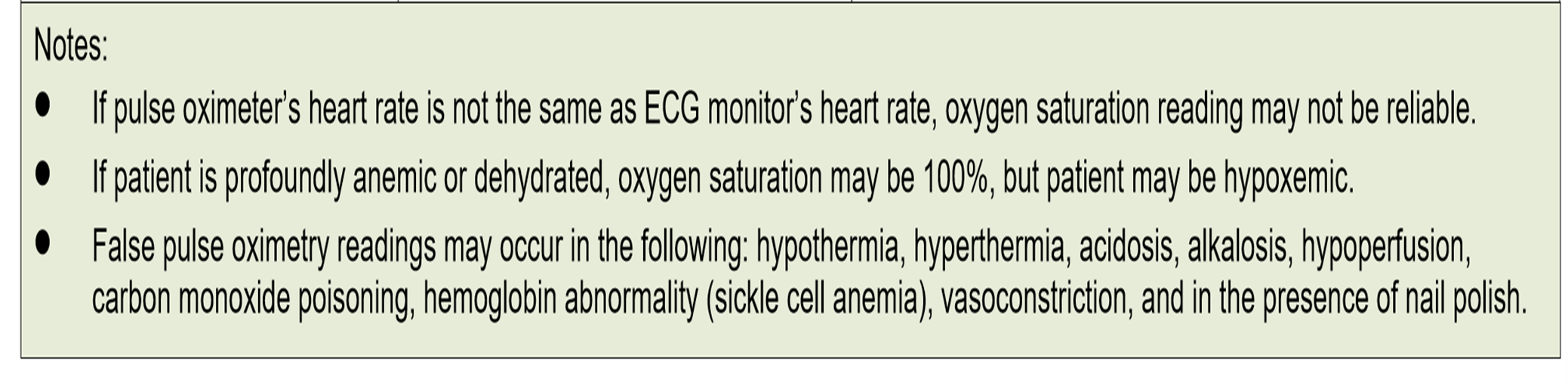
- Administer oxygen as appropriate with a target of achieving 94 % saturation (88 – 92% in COPD). CO- oximetry.
- Assess lung sounds and chest.
- Consider Advance Airway.
CIRCULATION ASSESSMENT
- Assess patient’s
pulse: -
pulse Present Yes No Speed Normal Slow Fast Regularity Regular Irregular
- Check pulse (feel for a pulse for at least 5 seconds but no more than 10 seconds), if no pulse or less than (60 beats/min for pediatric) Start CPR for 2 min, start
- Chest compressions (C-A-B Sequence) (30 compressions: 2 breaths) at a rate at least 100 compressions per minute.
- Assess patient’s Skin: -
| Skin | |||
| Tem | Warm | Hot | Cold |
| Color | Pink | Yellow | Red |
| Condition | Dry | Moist | |
- Assess patient’s Capillary Refill Time for pediatric: - (2 –seconds).
- Control bleedingusing direct pressure, pressure bandages, tourniquets.
- Establish IV access
and fluid resuscitation as appropriate for the patient’s
condition.
- For adult patients, administer fluids to maintain systolic blood
pressure refer to Shock Protocol – Adult (56 Medical).
- For pediatric patients, administer fluids based on physiological signs and therapeutic end-points refer to Shock Protocol – Pediatric (60 Medical).
- For adult patients, administer fluids to maintain systolic blood
pressure refer to Shock Protocol – Adult (56 Medical).
DISABILITY ASSESSMENT
- Assess level of consciousness appropriate for age; use (AVPU) Scale.
- If altered level of consciousness, check blood glucose.
- Utilize spinal motion restriction if indicated by assessment, see Advanced Spinal Assessment Procedure and Policy for Ault & Pediatric refer to Spinal Immobilization protocol (55 skills).
EXPOSE ASSESSMENT
- Remove the patient's cloths and take care of privacy.
TRANSPORT DECISION
- All patients should be transported to the closest appropriate Health Institutions (Hospital, Polyclinic, and Health Center).
- Regionalized systems of care for specialized trauma patients may necessitate transport to specialized center (Trauma, Burn Center).
- Notify receiving facility.
- Consider aeromedical transportation when indicated.
Secondary Assessment
SECONDARY/FOCUSED ASSESSMENT AND TREATMENT
- Reassess chief complaint, history of present illness.
- Complete a physical assessment as appropriate for the patient’s presentation.
| Trauma Patients | MOI | Ph/Exam (DCAPBTLS) | |
| Medical Patients | chief complaint, history of present illness | SAMPLE History |
Pain Assessment (OPQRST) (0 – 10) Scale. |
- Consider field diagnostic tests including: attach cardiac monitoring, obtain 3/12-lead ECG, blood glucose, body temperature, stroke assessment, pulse oximetry, etc.
- Check Pupil for light reaction.

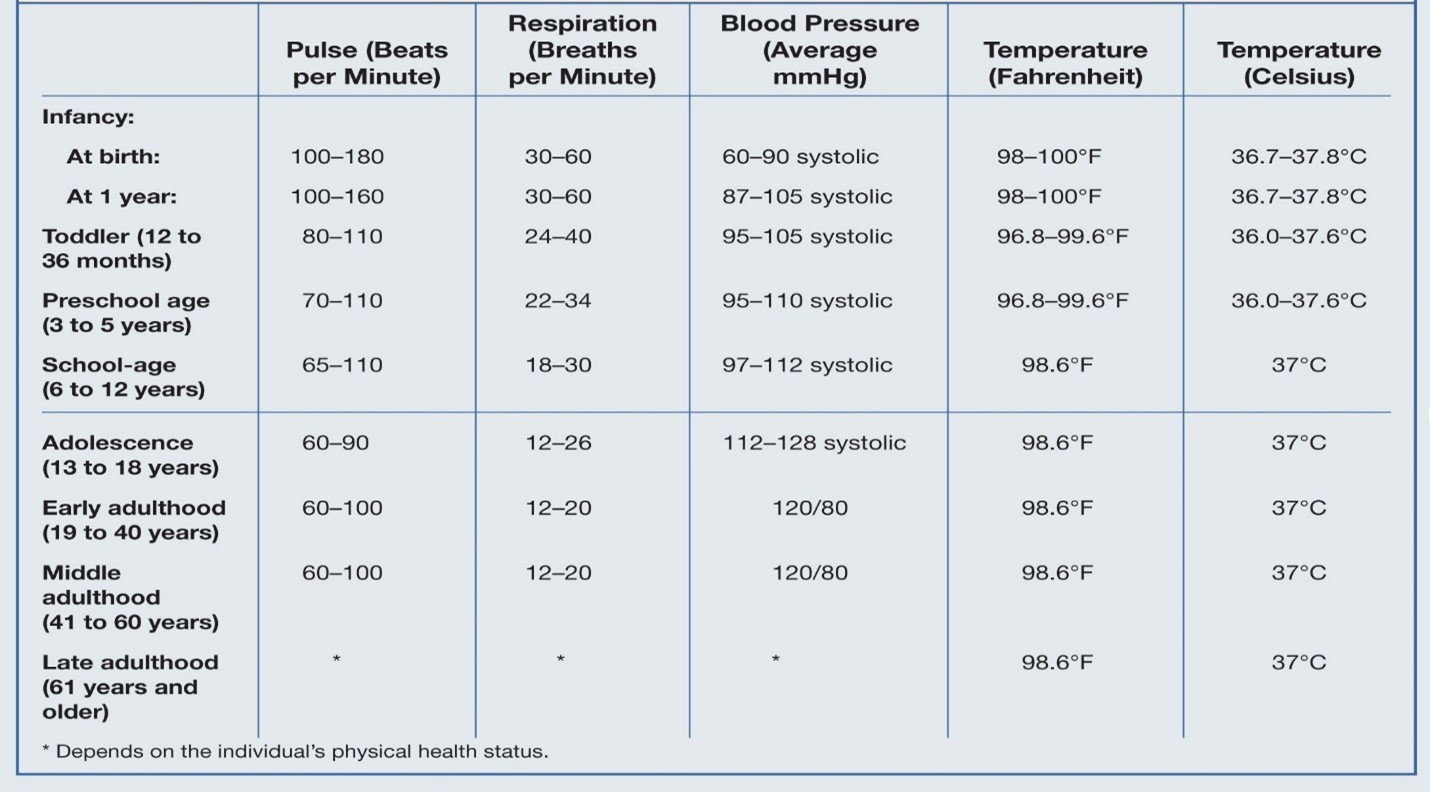
Take full set of vital signs. (it is the base set of vital signs).
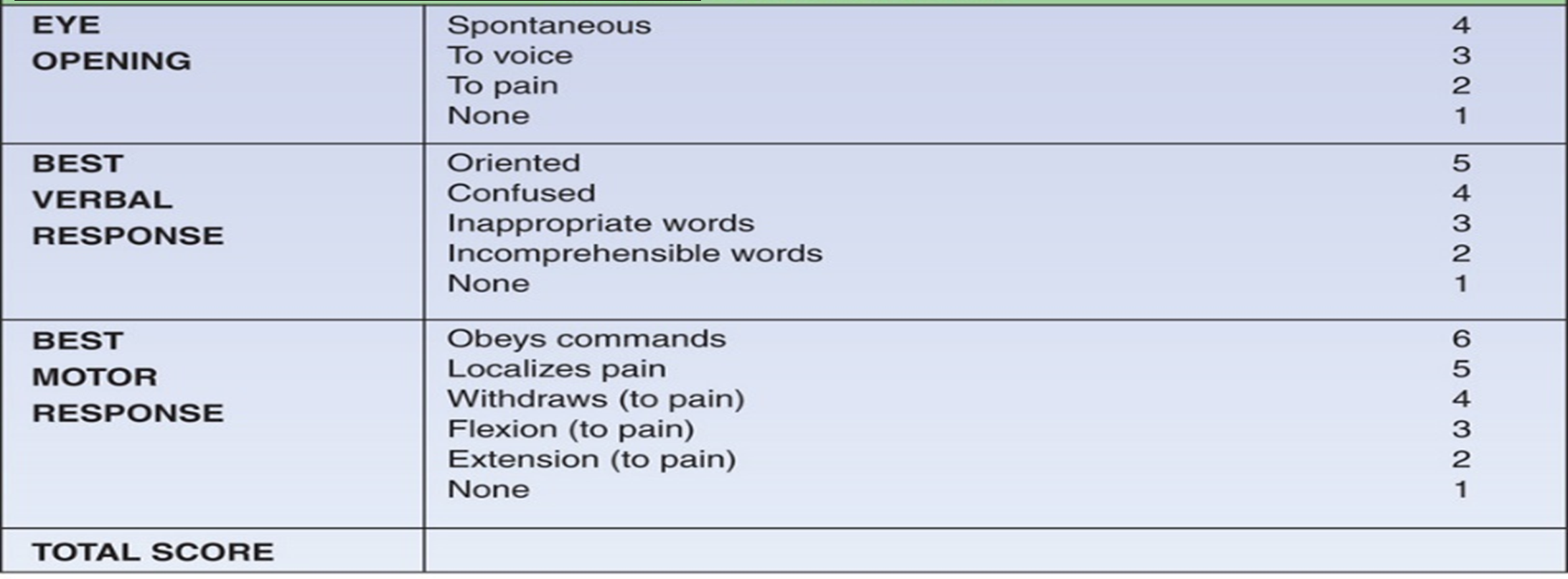
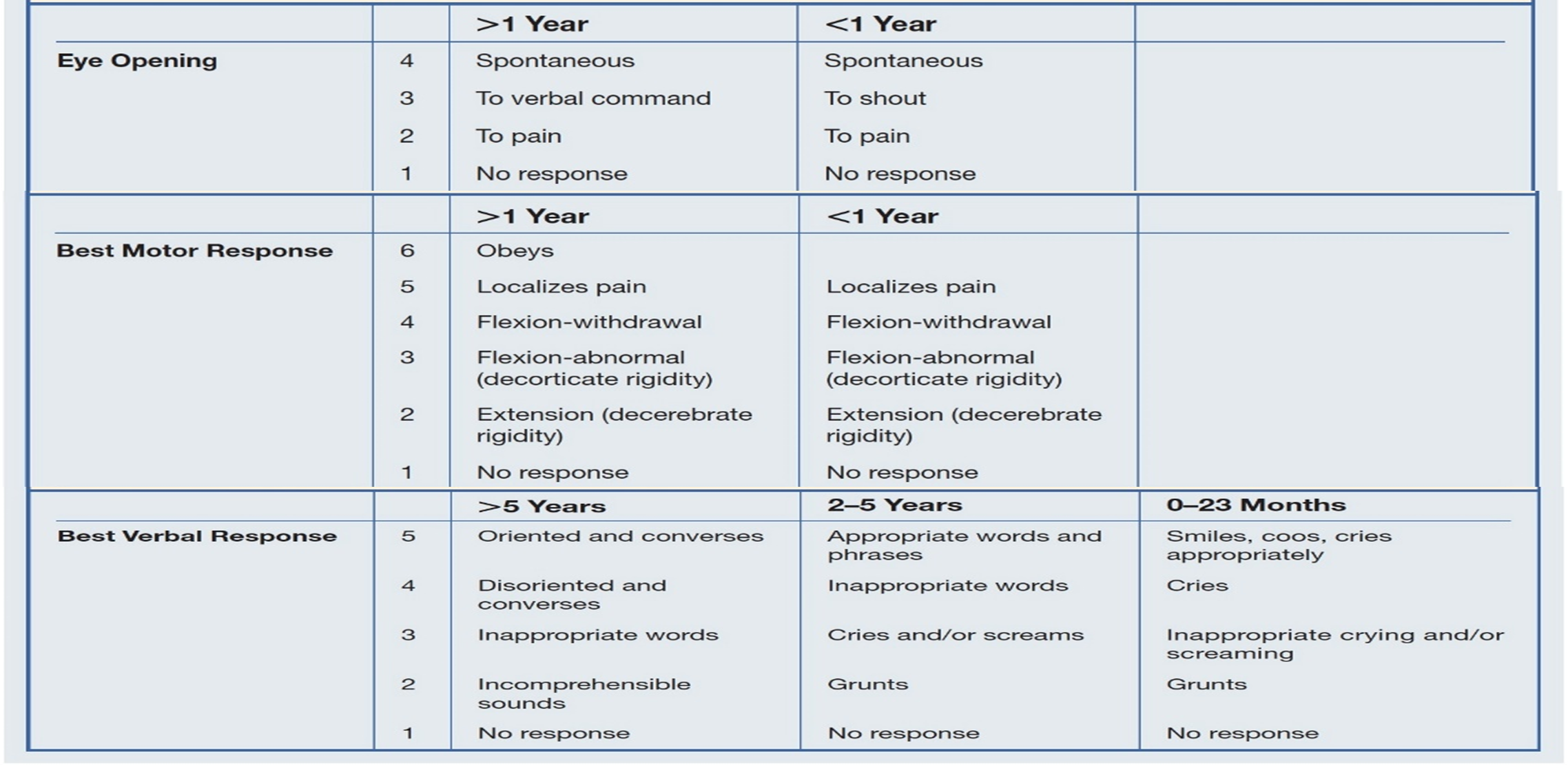
- Check disability by using Glasgow Come Scale.
-
Adult Glasgow Coma Scale
-
Pediatric Glasgow
- Refer to appropriate protocol(s) for further treatment options.
- Dress and bandage lacerations and abrasions.
- Cover evisceration with a sterile dressing to prevent heat loss.
- Maintain normal body temperature.
- Stabilize impaled objects. Do not remove an impaled object unless it interferes with CPR or your ability to maintain the patient’s airway.
- Recheck vital signs at least every 15 minutes (for stable patient) and at least every 5 minutes (for unstable patient).
TRAUMA SYSTEM
See Traumatic Emergencies Protocol (1 Trauma).