Syncope (Adult & Pediatric)
Syncope (Adult & Pediatric)
EMT STANDING ORDERS
- Routine Patient Care.
- Administer oxygen as appropriate with a target of achieving 94 - 98% saturation.
- Establish IV access.
- Attempt to determine the cause of syncope.
- Acquire and transmit 12-lead EKG, if available. If acute coronary syndrome is suspected, refer to Acute Coronary Syndrome Protocol - Adult (24 Cardiac).
- Obtain blood glucose analysis; refer to Diabetic Emergencies (Hyperglycemia) Protocol - Adult (7 Medical) or Pediatric (8 Medical), or Hypoglycemia Protocol - Adult (3 Medical) & Pediatric (5 Medical) if indicated.
- Patients with ongoing mental status changes or coma should be treated per the Altered Mental Status Protocol - Adult (16 Medical) or Pediatric (18 Medical).
- Perform stroke screening exam (See Stroke Protocol (56 Medical)).
- Assess for trauma either as the cause of the syncope or as a consequence of the syncopal event. Refer to Spinal Motion Restriction Protocol (14 Trauma), Traumatic Emergencies Protocol (27 Trauma) or Traumatic Brain Injury Protocol (20 Trauma) if indicated.
- Prevent and treat for shock; see Shock Protocol - Adult (56 Medical) or Pediatric (60 Medical).
- Consider ALS intercept.
ADVANCED EMT STANDING ORDERS:
- Establish IV access.
- Consider fluids per Shock Protocol - Adult (56 Medical) or Pediatric (60 Medical).
PARAMEDIC STANDING ORDERS
- Perform cardiac monitoring.
- Observe for and treat dysrhythmias as indicated.
PEARLS:
- Syncope is defined as a loss of consciousness accompanied by a loss of postural tone with spontaneous recovery.
- Consider all syncope to be of cardiac origin until proven otherwise.
- While often thought of as benign, syncope can be the sign of a more serious medical emergency. All patients with syncope deserve emergency department evaluation, even if they appear normal with few complaints on scene.
- Syncope that occurs during exercise often indicates an ominous cardiac cause. Patients should be evaluated at the ED. Syncope that occurs following exercise is almost always vasovagal and benign.
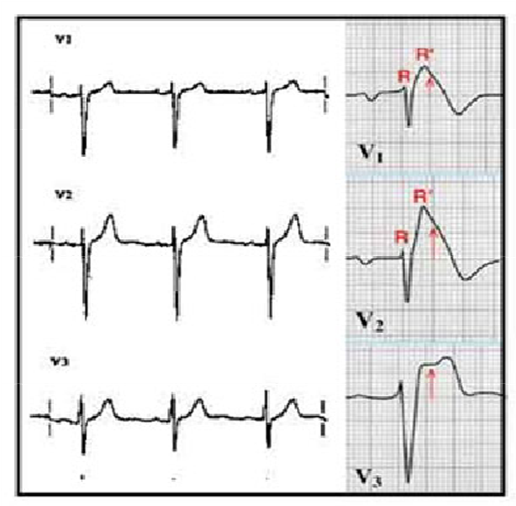
- Prolonged QTc (generally > 500ms), Brugada Syndrome (incomplete RBBB pattern in V1/V2 with ST segment elevation), Delta waves and hypertrophic obstructive cardiomyopathy should be considered in all patients.
- There is no evidence that supports acquiring orthostatic vital signs.
- Syncope can be indicative of many medical emergencies including:
- Myocardial infarction.
- Pulmonary embolism.
- Cardiac arrhythmias.
- Vasovagal reflexes.
- Diabetic emergencies.
- Aortic stenosis.
- TIA.
- Poisoning/drug effects.
- Dehydration.
- Hypovolemia.
- Seizures.
- Ectopic pregnancy.
- Stroke