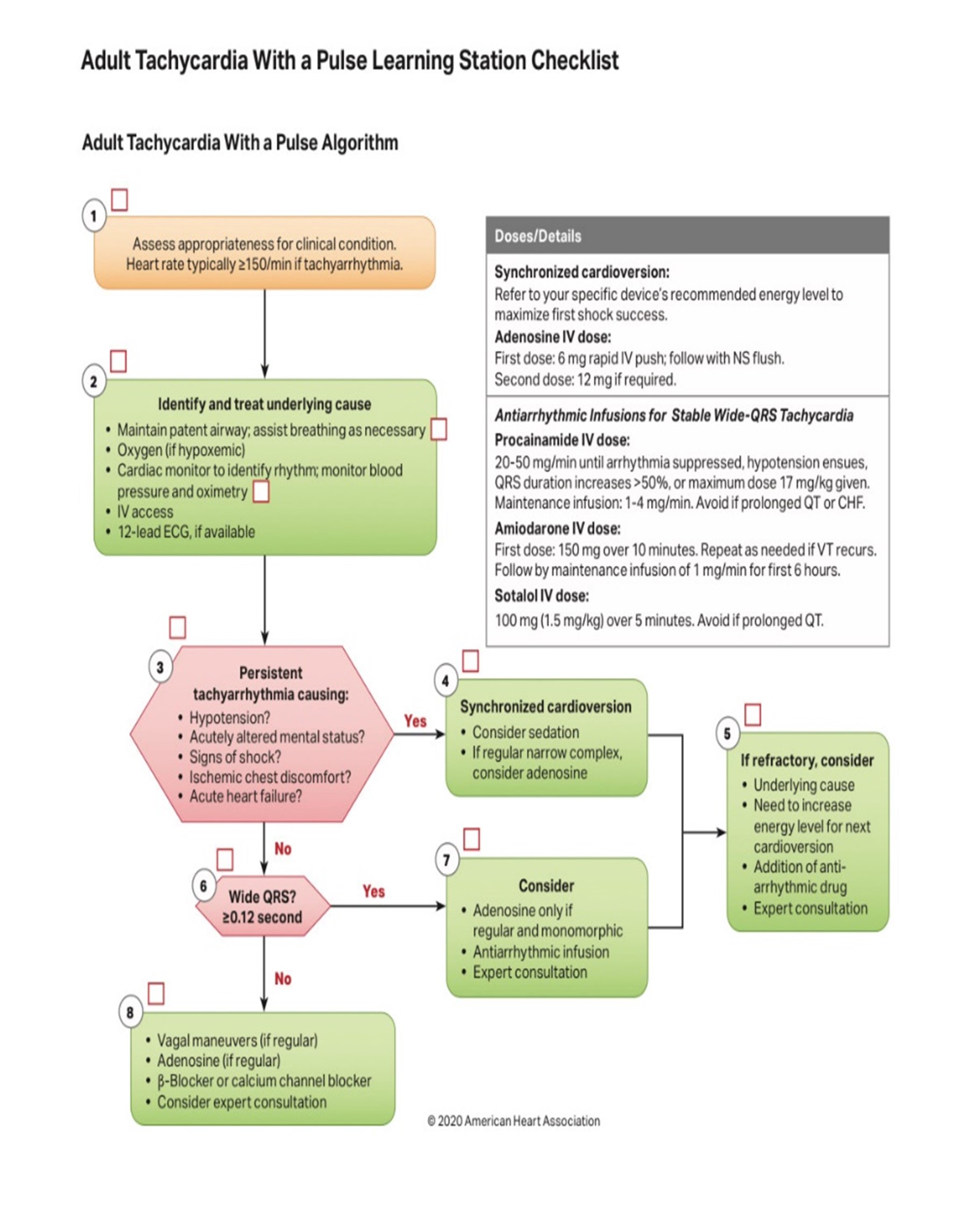
Tachycardia (Adult)
Tachycardia - Adult
EMT STANDING ORDERS:
- Routine Patient Care.
- If serious signs or symptoms (hypotension, acutely altered mental status, signs of shock, ischemic chest discomfort, or acute heart failure); Call for Paramedic intercept, if available.
- Obtain 3 lead ECG if available.
- Establish IV access to KVO.
- Call for AEMT/Paramedic intercept. & Assists AEMT/Paramedic in patient care.
AEMT/PARAMEDIC STANDING ORDER:
- Follow ACLS guidelines as trained and credentialed.
- Acquire and transmit 12-lead ECG, if available.
- If symptomatic and hemodynamically unstable:
- Consider cardioversion immediately.
- Consider procedural sedation prior to or during pacing:
- Midazolam 2-5 mg slow IV/IO, may repeat once in 5 minutes OR
- Diazepam 5 mg slow IV/IO, may repeat 5 mg once in 5 minutes.
- Use the following initial energy doses, then escalate to the next higher energy level if no conversion. (follow
manufacturer's recommendations for dosing).
- For narrow regular rhythm: 50 - 100J Biphasic or 200J monophasic.
- For narrow irregular rhythm: 120 - 200J Biphasic or 200J Monophasic.
- For wide regular rhythm: 100J Biphasic or Monophasic.
- For wide irregular/polymorphic VT: 200J Biphasic or 360 Monophasic, using unsynchronized defibrillation doses.
- If hemodynamically stable:
- For narrow complex tachycardia (with a heart rate persistently > 150 bpm):
- Attempt Vagal Maneuver, for regular rhythms.
If Vagal Maneuvers fail and the rhythm is regular:
- Adenosine 6 mg rapid IV/IO, followed by a rapid flush. May repeated once at a dose of 12 mg if no conversion.
- If irregular rhythm, to control ventricular rate:
- Diltiazem 0.25 mg/kg IV/IO (Maximum dose 20 mg) over 2 minutes. (Consider 10 mg maximum dose for elderly patient or patient with low BP.) May repeat dose in 15 minutes at 0.35 mg/kg (Maximum dose 25 mg), if necessary.
- Sotalol 100 mg (1.5 mg/kg) IV/IO over 5 minutes. Avoid if prolonged QT.
- For wide complex tachycardia:
- Only for regular rhythm with monomorphic QRS:
- Consider: adenosine 6 mg rapid IV/IO, followed by rapid flush.
- Amiodarone 150 mg IV/IO over 10 minutes. May repeat once in 10 minutes. If successful, consider a maintenance infusion of 1 mg/min OR
- Procainamide 20-50 mg/min IV/IO until arrhythmia suppressed. Maintenance infusion 1-4 mg/min. avoid if prolonged QT or CHF.
- Only for regular rhythm with monomorphic QRS:
- For polymorphic Ventricular Tachycardia/Torsade de Pointes: If pulse is present, consider magnesium sulfate1- 2 gm IV/IO diluted in 10 mL D5W or 0.9% NaCl over 10 minutes.
- Consider expert consultation.